
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Late pulmonary infarctus in patient with cardioMEMS pulmonary artery pressure sensor
Peggy Jacon1*; Antony Costa1; Aude Boignard1; Muriel Salvat1; Frederic Thony2; Pascal Defaye1
1 Department of Cardiology, University Hospital of Grenoble Alpes, 38043 Grenoble, France.
2 Department of Radiology, University Hospital of Grenoble Alpes, 38043 Grenoble, France.
*Corresponding Author: Peggy Jacon
Department of Cardiology, University Hospital of
Grenoble Alpes, 38043 Grenoble, France.
Email: PJacon@chu-grenoble.fr
Received : Jan 28, 2022
Accepted : Feb 21, 2022
Published : Feb 28, 2022
Archived : www.jcimcr.org
Copyright : © Jacon P (2022).
Abstract
A 63 year-old male with severe heart failure was implanted with a CardioMEMS™ pulmonary artery pressure sensor and received usual anti-aggregation therapy. Six months later, he was admitted for chest pain without respiratory or hemodynamic compromise. The CT-scan showed recent complete thrombosis of the pulmonary branch downstream of the CardioMEMS™. His progression was favorable under curative anticoagulation. Data from the sensor remained usable without significant variation during the episode. Late pulmonary events can occur in the presence of a CardioMEMS™ device. Thus use of a CardioMEMs device should be carefully discussed, particularly when systematic anticoagulation is not possible.
Citation: Jacon P, Costa A, Boignard A, Salvat M, Thony F, et al. Late pulmonary infarctus in patient with cardioMEMS pulmonary artery pressure sensor. J Clin Images Med Case Rep. 2022; 3(2): 1698.
Introduction
The CardioMems™ pulmonary artery sensor (CardioMEMS™ HF System, Abbott, Atlanta, GA, USA) can be proposed for severe heart failure management even in patients awaiting heart transplantation or implanted with a left ventricular assist device. Its usefulness and short-term safety profile¹ have been well demonstrated, but long-term safety remains not well known. We present the case of a patient who developed a late pulmonary thrombosis possibly linked to a CardioMEMS™ sensor.
Case report
A 63 year-old male suffering from severe heart failure due to ischemic cardiomyopathy (myocardial infarction in 2003) was referred to our unit in December 2020 to discuss heart transplantation and a left ventricular assist device in the interim period. He had remained symptomatic (NYHA class 3) despite maximal medical therapy (160 mg aspirin, 40 mg furosemide, 10 mg bisoprolol, 24/26 mg sacubitril/valsartan and 12.5 mg spironolactone daily) and after resynchronization therapy (ICDCRT). Transthoracic echography showed a left ventricular ejection fraction of 20% with left ventricular end-diastolic diameter 73 mm and moderate dilation of the right cavities. The right catheterization showed a pulmonary artery pressure 55/20 mmHg (mean 20), PCWP 18/28 mmHg (mean 25), Qc 4.4 L/min, cardiac output 2 L/min/m2 and pulmonary vascular resistance 1.1 UW.
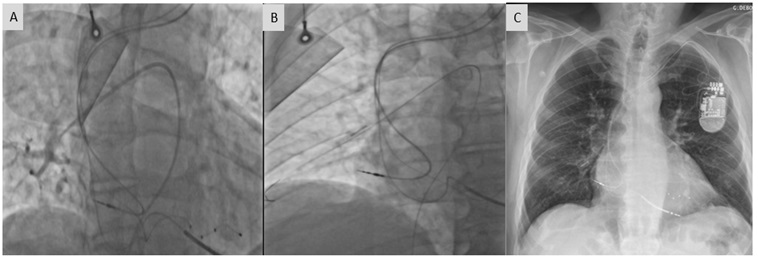
During the examination, the patient was referred for implantation of a CardioMEMS™ pulmonary artery pressure sensor. This indication was validated by the heart failure team. The procedure was performed under conscious sedation. Angiography of the left pulmonary arteries found no ideal area for positioning of the device due to the small diameter of the branches. A lobar right pulmonary branch of 8 mm diameter was considered acceptable and the CardioMems™ sensor was implanted here using a Nitrex™ 0.018-inch guide-wire for support (Figure 1). Per-operative measurements confirmed good correlation between hemodynamic and sensor measurements. There were no postoperative complications.
The patient was discharged with the usual mono anti-aggregation (160 mg aspirin per day) regimen. At the 3-month follow-up, the injected CT-scan performed for pulmonary pretransplantation evaluation revealed no abnormalities relative to the device.
In June 2021, 6 months after sensor implantation, the patient was re-admitted for retrosternal chest pain and dyspnea. An initial evaluation confirmed persistent moderate chest pain, usual hemodynamic measurements, 95% saturation, BNP 239 pg/mL, normal troponin, and a positive D-dimer measurement. Transthoracic echography showed no significant change compared to previous examinations, especially regarding right ventricle function. A CT-scan revealed thrombosis of the basal segmental branch of the pulmonary artery (A8-ç trunk of right inferior lobe) just downstream of the sensor (Figure 2). Pulmonary condensation in the area was considered to be linked to a recent pulmonary infarction. No deep venous thrombosis was detected, nor coagulation abnormalities.

Under oral anticoagulation (5 mg apixaban twice a day) the patient’s progression was favorable and he was discharged 2 days later.
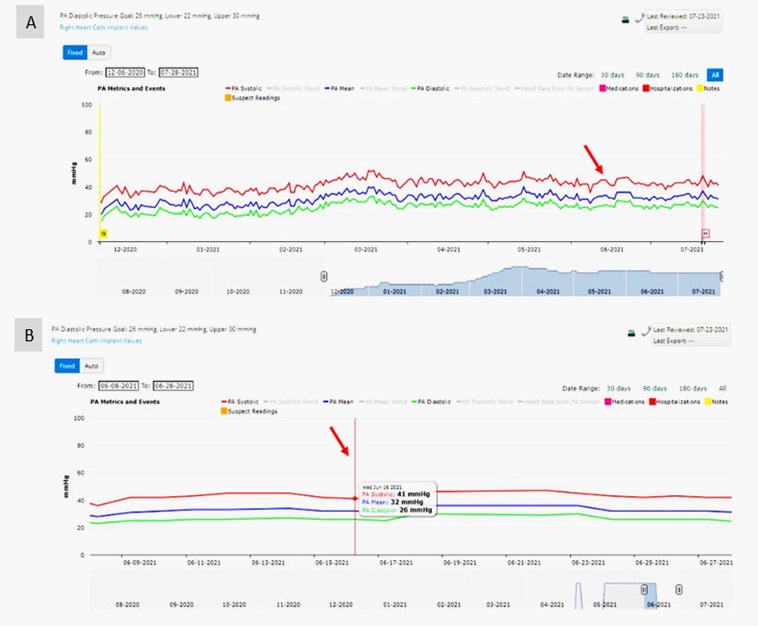
The sensor data (uninterrupted throughout the episode) were reevaluated for the month preceding and close to the event, but no significant variation in the measurements was detected (Figure 3). At the one-month follow-up the D-dimer measurement was negative suggesting no worsening of the thrombotic process.
Discussion
The main observations from this case were: (1) the CardioMEMS™ sensor might have led to pulmonary thrombosis; (2) this occurred in the chronic phase after device implantation; (3) pulmonary thrombosis downstream of the device appeared not to compromise the sensor’s efficacy; and (4) sensor measurements seemed not fluctuate even in the presence of thrombosis in the area of the device.
The CardioMEMS™ pulmonary artery pressure sensor is reputed for its usefulness for monitoring of severe heart failure. It has been evaluated in a RCT, the CHAMPION trial [1], which included 550 patients with severe heart failure (NYHA grade III) and hospitalization in the previous year, using a 6-month efficacy endpoint (reduction in the rate of hospital admissions). Safety issues were also studied throughout the 18 month follow-up. Regarding thrombotic events: only one in-situ thrombus was reported in the operative step, and was treated by oral anticoagulation. An ancillary open-label study [2], after13 months additional follow-up, performed at the request of the FDA, showed no further system-related events (0.02 events per patient-year in the entire follow-up period). However, these mid-term data were collected for a reduced sample size at 31 months (24/550), which could have led to a possible loss of information in terms of safety. After one-year follow-up, the observational studies PAS-US³ and MEMS-HF [4] showed respectively 98.3% and 99.6% freedom from device- or system-related complications or sensor failure. The COAST-UK [5] results are expected to confirm this excellent safety profile. However, no data has been published on long-term tolerance to the sensor.
To our knowledge, this is the first report of a thrombotic event that is possibly directly attributed to CardioMEMS, although the site of the pulmonary thrombosis leaves little doubt as to a direct link with the device. The clinical examinations, biological laboratory results and imaging data, as well as the previous normal CT-scan, show that the event occurred late (at over six months) after device implantation. No other disorders were associated with the case, particularly no hemostasis abnormalities. However, it is usually recommended to use dual anticoagulation therapy in the first month post-implantation followed by long-term mono anti-aggregation or anticoagulation therapy. In the present case the patient was on mono anti-coagulant before, and long-term after device implantation, including immediately after the intervention when dual anticoagulation is usually recommended. How relevant this is may be debatable as the thrombotic event occurred quite some time after the intervention.
This case may raise questions about the long-term tolerance of the CardioMEMS™ device by this fragile heart failure population. While curative anticoagulation is not mandatory during CardioMEMS™ follow-up, it is widely prescribed for heart failure patients and should be considered for all CardioMEMS™ recipients. Moreover, some patients have sensors implanted in the bridging period before heart transplantation and the absence of a perfect safety profile can be a problem. In case of bridging before left ventricular assist device as the destination therapy, pulmonary thrombotic events can lead to dysfunction of the right ventricule and could jeopardize the implantation.
This case should force us to reconsider CardioMEMS™ safety especially for high-risk patients who are candidates for heart transplantation and/or a left ventricular assist device.
In the present case, we observed perfect stability in the measurements given by the device even around the thrombotic event. This might be explained by the sensor being positioned downstream of the affected area. The absence of fluctuation might suggest that the hemodynamic status of this patient was little compromised by the thrombosis and/or was already deteriorated. It is thus important to be aware of the risk of pulmonary thrombosis in CardioMEMS™ recipients, particularly those who do not receive dual anticoagulant therapy during the immediate post-implantation period. It is difficult to draw conclusions from a single case report, and any further suspect cases should be immediately reported. In the meanwhile we suggest curative anticoagulation for these advanced heart failure patients.
References
- Abraham WT, Adamson PB, Bourge RC, Aaron MF, Costanzo MR, Stevenson LW, et al. CHAMPION Trial Study Groupl. Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: a randomised controlled trial. The Lancet. 2011 Feb.
- Abraham WT, Stevenson LW, Bourge RC, Lindenfeld JA, Bauman JG, Adamson PB. CHAMPION Trial Study Group. Sustained efficacy of pulmonary artery pressure to guide adjustment of chronic heart failure therapy: complete follow-up results from the CHAMPION randomised trial. The Lancet. 2016; 387(10017): 453-61
- Shavelle DM, Desai AS, Abraham WT, Bourge RC, Raval N, Rathman LD, et al. CardioMEMS Post-Approval Study Investigators. Lower Rates of Heart Failure and All-Cause Hospitalizations During Pulmonary Artery Pressure-Guided Therapy for Ambulatory Heart Failure: One-Year Outcomes From the CardioMEMS Post-Approval Study. Circ Heart Fail. 2020; 13(8): e006863. doi: 10.1161/CIRCHEARTFAILURE.119.006863. Epub 2020 Aug 6.Circ Heart Fail. 2020. PMID: 32757642.
- Angermann CE, Assmus B, Anker SD, Asselbergs FW, Brachmann J, Brett ME, et al. MEMS-HF Investigators. Pulmonary artery pressure-guided therapy in ambulatory patients with symptomatic heart failure: the CardioMEMS European Monitoring Study for Heart Failure (MEMS-HF). Eur J Heart Fail. 2020; 22(10): 1891-1901. doi: 10.1002/ejhf.1943. Epub 2020 Aug 9.Eur J Heart Fail. 2020. PMID: 32592227.
- Martin R Cowie, Pascal de Groote, Scott McKenzie, Marie-Elena Brett, Philip B Adamson, et al. CardioMEMS Post-Market Study Investigators Rationale and design of the CardioMEMS PostMarket Multinational Clinical Study: COAST ESC Heart Fail . 2020; 7(3): 865-872.