
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
An unfamiliar outcome of a familiar case presentation: Severe aortic stenosis and type-2 myocardial infarction
Ashwini P Sadhale, MD1*; Mandip S Kang, MD1; Angela Sehgal, MD1; Gurjap S Dhaliwal, MD1; Manminder Bhullar, MD2
1 Department of Internal Medicine, UCSF Fresno, Fresno, California, USA.
2 Department of Cardiovascular Disease, UCSF Fresno, Fresno, California, USA.
*Corresponding Author: Ashwini Parag Sadhale
Department of Internal Medicine, UCSF Fresno,
Fresno, California, USA.
Email: asadhale@fresno.ucsf.edu
Received : Jan 29, 2022
Accepted : Feb 22, 2022
Published : Mar 01, 2022
Archived : www.jcimcr.org
Copyright : © Sadhale AP (2022).
Abstract
Management of cardiogenic shock is complex. It’s important to know the underlying mechanism. Two of many underlying mechanisms are critical aortic stenosis and Type-1 NSTEMI. Aortic stenosis can rarely present with a troponin leak high enough to resemble a Type-1 NSTEMI, making it hard to diagnose aortic stenosis early.
Keywords: cardiogenic shock; ischemia; elevated troponin; NSTEMI.
Abbreviations: NSTEMI: non-ST elevation myocardial infarction; LVH: Left ventricular hypertrophy; MI: Myocardial infarction; EKG: Electrocardiogram; AS: Aortic stenosis; SAVR: Surgical aortic valve replacement; LVEDP: Left ventricular end diastolic volume.
Citation: Sadhale AP, Kang MS, Sehgal A, Dhaliwal GS, Bhullar M. An unfamiliar outcome of a familiar case presentation: Severe aortic stenosis and type-2 myocardial infarction. J Clin Images Med Case Rep. 2022; 3(3): 1700.
Introduction
A 59-year-old male with no significant past medical history presented to an outside hospital with complaints of shortness of breath and chest pain that had been going on for 2-3 days. On initial presentation, he was found to be in hypoxic respiratory failure with significant pulmonary edema and an elevated troponin I of 99. He was placed on Bilevel Positive Airway Pressure (BiPAP) and given Lasix without improvement, subsequently requiring him to be intubated and transferred to a tertiary hospital for further care. En route he became hypotensive, started on norepinephrine, got intubated for hypoxemia and presented to our institution on 15 mcg/min of norepinephrine. He was neurologically intact and able to follow commands, noted to have jugular venous distention, pink frothy sputum in the endotracheal tube, bilateral crackles and systolic murmur without any overt radiation. At this point the patient was transitioned to a dobutamine drip at a fixed dose, started on bumetanide drip and was admitted to the medical intensive care unit with a working diagnosis of cardiogenic shock secondary to type 1 NSTEMI.
PMH: No significant past medical history.
Differential: Cardiogenic shock secondary to Type 1 NSTEMI, Type 2 NSTEMI, Mitral regurgitation or Aortic stenosis.
Investigation
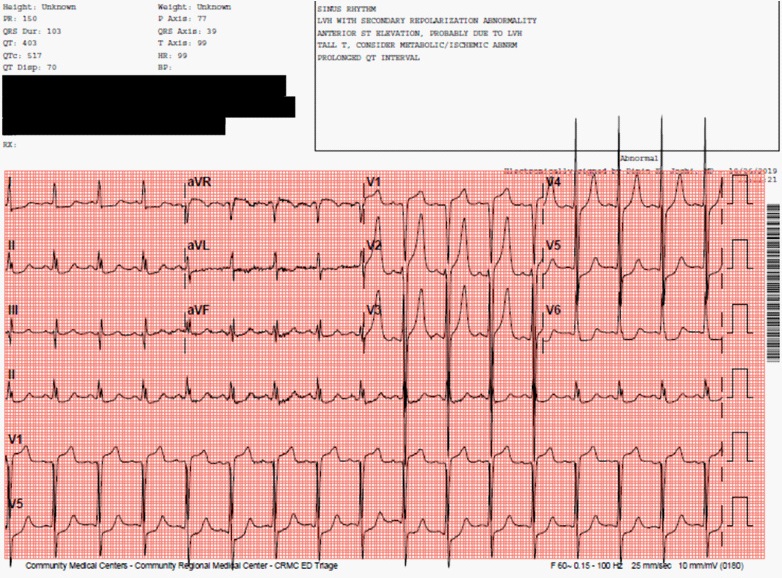
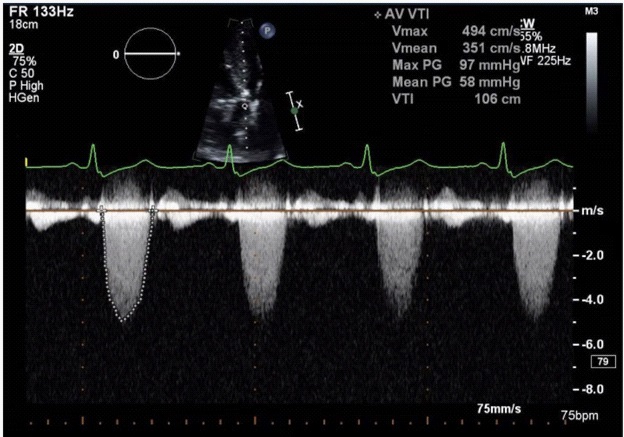
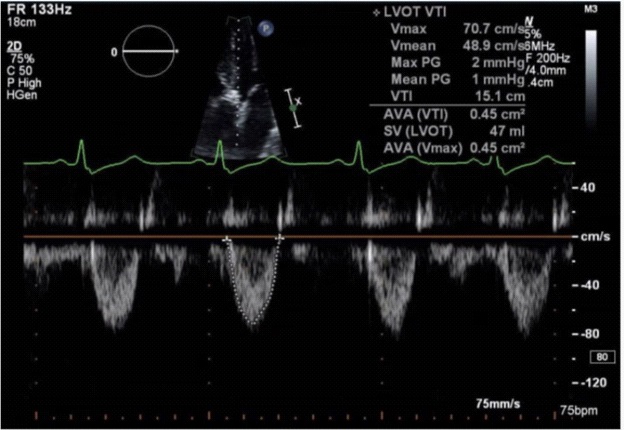
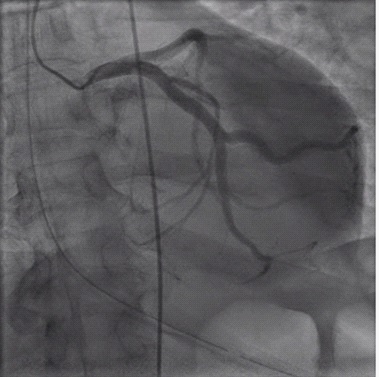
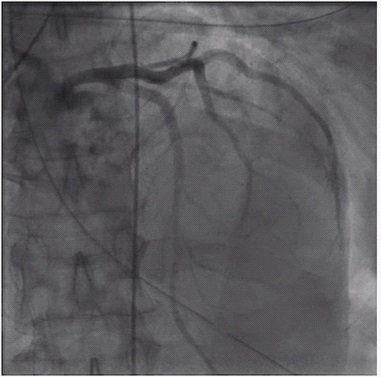
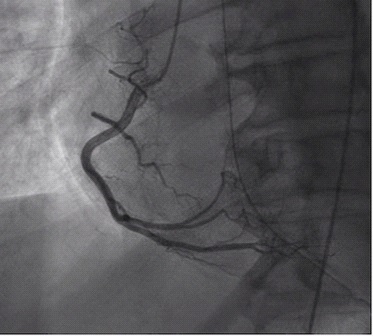
EKG was consistent with left ventricular hypertrophy (LVH) with associated repolarization changes, diffuse ST depression and tall T waves with concern for global ischemia. Troponin was 264 nanograms/milliliter (up from 99 nanograms/milliliter from the initial primary center) and peaked at 284.8 nanograms/milliliter. The transthoracic echocardiogram showed critical aortic stenosis with peak velocity of 4.94 m/s, mean pressure gradient of 58 mmHg, aortic valve area of 0.45 cm2 , severe LVH and left ventricle ejection fraction of 50-55%. He subsequently underwent an emergent left heart catheterization which showed angiographically normal coronary arteries. It was clear that this was cardiogenic shock secondary to critical aortic stenosis causing significant hypoperfusion of the severely hypertrophied left ventricle leading to type 2 MI (Figures 1-6).
Management
Shortly after the arrival of the patient to our tertiary care center, the patient was admitted to the medical intensive care unit and continued on vasopressor support with norepinephrine, dobutamine and was started on bumetanide drip for diuresis. The initial treatment was based on all physical exam findings (Acute hypoxic respiratory failure, positive Jugular Venous Distension, Mild lower extremity edema, hypotension) and diagnostic findings (Electrocardiogram findings, progressively increasing troponin I levels) all of which were thought to be from cardiogenic shock secondary to type 1 NSTEMI. On confirming the diagnosis to be type 2 MI in setting of critical AS and not type 1 NSTEMI with the help of the Echocardiogram and Left Heart Catheterization, the patient had an urgent Surgical Aortic Valve Repair (SAVR) with in 24 hours of presentation with a 25 mm Trifecta bioprosthetic aortic valve
Discussion
Aortic stenosis affects 2-9% of the population above the age of 65 and increases proportionately with aging [1]. Severe aortic stenosis is defined by a transvalvular gradient of 40 mmHg, an aortic jet velocity of 4 m/s and an aortic valve area of <1 cm2 [2]. Patients with aortic stenosis are found to have a higherthan-normal level of trop I with mean levels 0.07+/- 0.02 compared with a mean value of 0.01+/- 0.02 in people without any cardiovascular disease [3]. This is thought to be related to the possibility that stimuli leading to cardiac hypertrophy can cause increased release of troponin I or that increased left ventricular (LV) wall thickness could cause increase in apoptosis of the cardiac myocytes [3]. The pathophysiology of ischemia in AS is multifactorial and complex.
Severe aortic stenosis is associated with structural remodeling in the myocardium in addition to alteration of the hemodynamics of the coronary circulation [4]. The chronic pressure overload of the LV from the AS leads to significant concentric hypertrophy and elevation in LV end diastolic pressure (LVEDP) [4]. AS is also associated with a reduction in the aortic diastolic pressure [2]. The combination of increased LVEDP and reduced aortic diastolic pressure reduces the coronary perfusion pressure gradient [2]. A hypertrophied LV also has increased oxygen demand which is met by increased total blood flow at rest by metabolic vasodilation of the microcirculation[4]. This results in the exhaustion of coronary autoregulation and a lowered coronary vasodilator reserve [4]. In addition, AS is also associated with increased LV ejection time and reduced diastolic time equivalent to myocardial perfusion time [2]. Diastolic coronary flow progresses from the subepicardium to the subendocardium causing selective impairment of subendocardial perfusion [4]. All the above mechanisms can predispose patients to ischemic complications.
There are no specific guidelines and the patients in cardiogenic shock secondary to AS require individualized and challenging treatment. They are best supported by phenylephrine due to its pure alpha 1 agonistic property which causes an increase in diastolic blood pressure leading to increased coronary perfusion and reflex bradycardia (increasing diastolic time). Fluid balance has to be carefully maintained as even minute changes in the volume status can affect cardiac output. Liberal diuresis can lead to deleterious effects in the setting of AS. Definitive management is surgical or percutaneous aortic valve replacement. In our patient, despite the presence of an ejection systolic murmur on exam we continued to treat the patient initially as a case of type 1 NSTEMI due to the extremely high troponin I value till we had a left heart catheterization report. The liberal diuresis and use of dobutamine as an inotrope could have been deleterious to the patient had they not been stopped in time. This emphasizes the importance of realizing that extremely high levels of troponin can be found in aortic stenosis in the absence of significant coronary artery disease and we must have a high level of suspicion.
Follow up
The patient was discharged on the ninth day of hospitalization. He has been symptom free. Was seen twice at the outpatient clinic without any complaints at 1 and 6 month follow up visits.
Conclusion
Though a rare cause of troponin elevation, it is important to keep aortic stenosis in mind as one of the differential diagnoses. This case also highlights the importance of physical exam and early investigation using non-invasive methods like the echocardiogram. The mechanism of ischemia in aortic stenosis is complex and not completely understood yet. Managing cardiogenic shock in the setting of aortic stenosis needs individualized treatment with extremely close monitoring and fine fluid balances. In addition to this we would also like to highlight such an elevated troponin with critical AS, as this does not seem to be reported in any of the literature that we are aware of.
Learning objectives
1. To recognize that critical aortic stenosis is an important cause for Type-2 MI leading to cardiogenic shock 2. The management of cardiogenic shock is complex and needs to be tailored based on every individual patient.
Declarations
Disclosures: The authors have nothing to disclose
Funding: The authors received no funding
References
- Gue YX, Bhandari SS, Kelly DJ. Critical aortic stenosis presenting as STEMI. Echo Res Pract. 2017; 4(3): K7-K10. doi:10.1530/ERP17-0017
- Douglas P. Zipes & Peter Libby & Robert O. Bonow & Douglas L. Mann & Gordon F Tomaselli. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. Volume 2, 11th Edition.
- Nunes, José Pedro L., et al. “Cardiac Troponin I in Aortic Valve Disease.” International Journal of Cardiology. 2003; 89(2-3): 281-85. DOI.org (Crossref), doi:10.1016/S0167-5273(02)00502- 8.
- Cardiac arrest due to critical stenosis of a bicuspid aortic valve mimicking left main coronary artery occlusion on ECG. Abhinav Saxena, Nitin Sabharwal, Bernard Topi, Gregory Crooke.
- Huang, Tien-Chi, et al. “Diffuse ST-Segment Depression with ST-Segment Elevation in Lead AVR in 12-Lead Electrocardiography May Indicate Ischemic Change of Severe Aortic Stenosis.” Acta Cardiologica Sinica. 2015; 31(5): 449-52. PubMed Central, doi:10.6515/ACS20140813A.