
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Nonpuerperal mastitis associated with prolactinoma: Case report
Minhui Tang1,2,3; Wenhe Huang1,2,3*
1 Xiang’an Hospital of Xiamen University, The Department of Breast-Thyroid Surgery, China.
2 Xiamen Research Center of Clinical Medicine in Breast & Thyroid Cancers, China.
3 Xiamen Key Laboratory of Endocrine-Related Cancer Precision Medicine, China.
*Corresponding Author: Wenhe Huang
Xiang’an Hospital of Xiamen University, The Department of Breast-Thyroid Surgery, China.
Email: t8515460a@163.com
Received : Jan 31, 2022
Accepted : Feb 24, 2022
Published : Mar 03, 2022
Archived : www.jcimcr.org
Copyright : © Huang W (2022).
Abstract
Nonpuerperal mastitis (NPM) is characterized by chronic nonspecific inflammation, complex pathological types, and unclear causes. Prolactin seems to play an important role in the occurrence and development of NPM. This study reports two cases of mastitis with prolactinoma. While treating mastitis, active treatment of prolactinoma and reduction of prolactin levels have achieved good curative effects.
Keywords: non-puerperal mastitis; prolactinoma; hyperprolactinemia.
Abbreviations: NPM: nonpuerperal mastitis; CRP: C-reactive protein; RF: rheumatoid factor; ANAs: antinuclear antibody spectrum; PDM: periductal mastitis; GLM: granulomatous lobular mastitis.
Citation: Tang M, Huang W. Nonpuerperal mastitis associated with prolactinoma: Case report. J Clin Images Med Case Rep. 2022; 3(3): 1708.
Introduction
Nonpuerperal mastitis (NPM) is characterized by the presence of chronic inflammatory disease. It often occurs in women during the non-lactation period and has a history of pregnancy [1]. The etiology of NPM is unclear, and the treatment process is long, which seriously affects patient quality of life. Some experts consider that NPM is a type of autoimmune disease, which may be related to lactation factors, Corynebacterium kroppenstedtii infection, and trauma, etc [2]. The following cases are of two female patients who were diagnosed with NPM and pituitary prolactinoma in the Xiang’an Hospital of Xiamen University
Case reports
Case 1
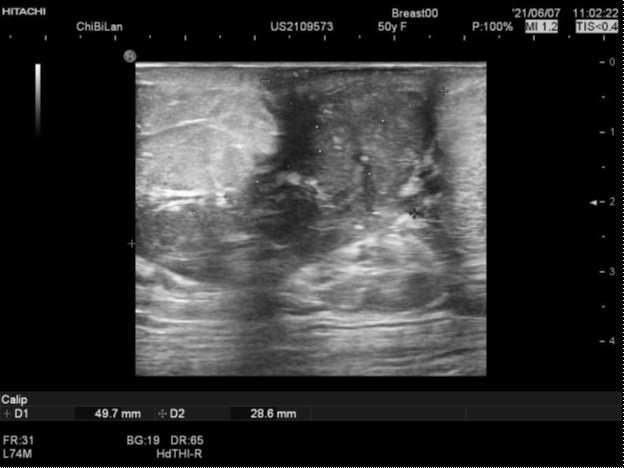
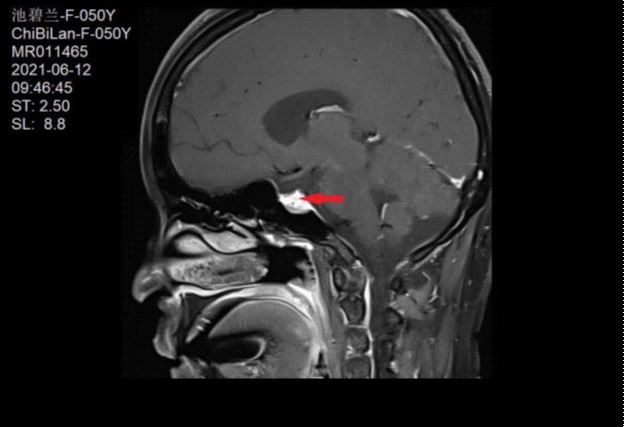
A 50-year-old female patient presented with right nipple ulceration with purulent discharge, redness and pain in the areolar area lasting for five days (Figure 1). She denied having any fever or trauma to the breast. No significant improvement was observed after oral cefuroxime treatment. She had menarche at the age of 14 years, and irregular menstrual cycles. She was currently in perimenopause. Upon examination, the sedimentation rate was high (25 mm/h), CA 125 was high (36.5 U/m), and prolactin was high (8038 mlU/L). The leukocyte count, Creactive protein (CRP), rheumatoid factor (RF), immune-related indices (C3, C4, IgG, IgA, and IgM), antinuclear antibody spectrum (ANAs), and thyroid function were all within the normal range. Breast ultrasound showed irregular solid heterogeneous hypoechoic mass lesions of 5.0 cm X 2.9 cm, suspicious for malignancy, or inflammation and abscess. Inflamed lymph nodes were observed in the right axilla (Figure 2). Aerobic and anaerobic abscess cultures did not produce any microorganisms, including Corynebacterium kroppenstedtii. Due to hyperprolactinemia, enhanced brain MRI revealed a pituitary macroadenoma close to the internal carotid artery (Figure 3). After neurosurgery, endocrinology and ophthalmology consultations, there was no indication for surgery. Bromocriptine (2.5 mg/day) was given to the patient. After one month, the prolactin level decreased to 572 mlU/L, nipple ulceration healed, and redness was significantly reduced. Then, the patient underwent surgery, and pathological examination revealed periductal mastitis (PDM) (Figure 4).

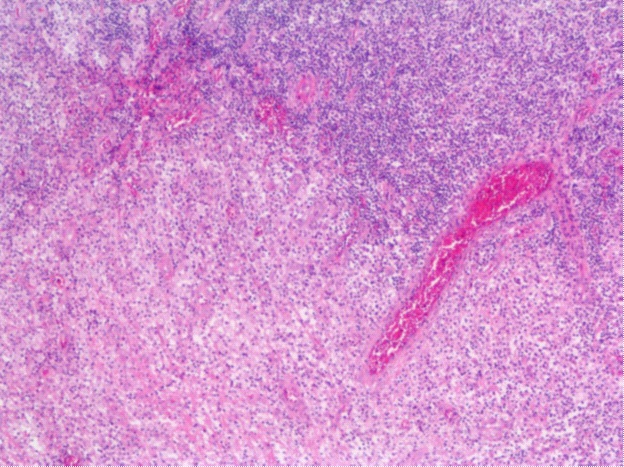
Extensive catheter dilation, partial catheter rupture, and secretion overflow were seen. While infiltration of peripheral lymphocytes and foam cells was observed, the patient did not show multinucleated giant cells and plasma cells.
Case 2
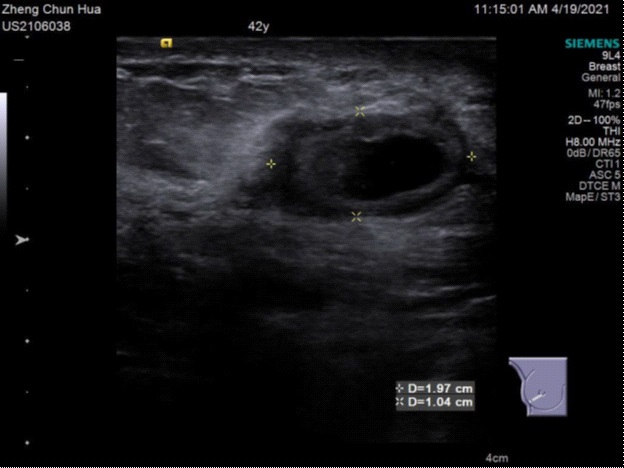
A 42-year-old female patient presented with a mass, ulceration, and abscess formation in her right breast that had persisted for 2 days. No fever or trauma to the breast were noted. She had menarche at the age of 15 years, and irregular menstrual cycles. She was diagnosed with pituitary microadenoma seven years prior to the study and treated with bromocriptine. However, she had stopped taking drugs of her own volition because of an inability to tolerate side effects, such as dizziness. Upon examination, prolactin level was high (2585 mlU/L). Leukocyte count, CRP, sedimentation rate, RF, immune-related indices, and ANAs were all within the normal range. Breast ultrasound showed two heterogeneous hypoechoic areas in the outer and lower quadrants of the breast, with respective sizes of 3.9 cm X 0.8 cm and 2.0 cm X 1.0 cm. The two lesions were connected, with a clear boundary, a regular shape, and an echo-free area inside. There were no lymph nodes in either axilla (Figure 5). A biopsy is recommended for the differential diagnosis of inflammatory and breast cancer. Core biopsy of the right breast mass revealed inflammatory lesions of mastitis, with local abscess formation and focal fibrous tissue hyperplasia (Figure 6). Special staining, including PSA, silver hexamine, and acid-fast staining, did not show any pathogens. Abscess cultures did not grow any microorganism, including C. kroppenstedtii. After anti-inflammatory, prolactin inhibitor, and steroid treatment, she underwent breast abscess incision and drainage, and the abscess cavity wall was removed at the same time. Pathological examination revealed local lymphocyte and plasma cells infiltration with tissue cells aggregation, which is consistent with granulomatous lobular mastitis (GLM) diagnosis in clinical practice.
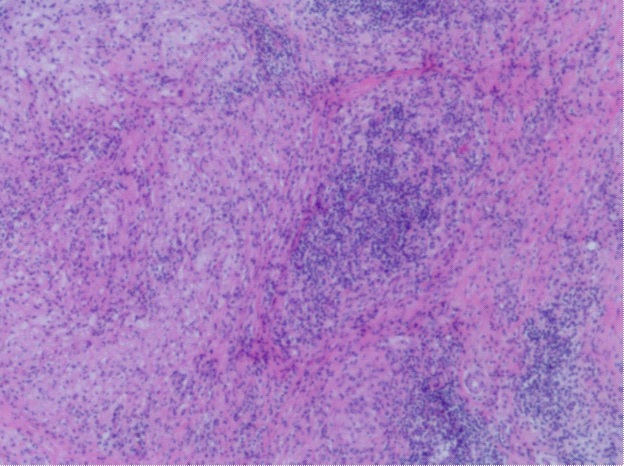
Histopathology showing benign breast tissue with marked acute and chronic inflammation, and the presence of a small abscess.
Discussion
In recent years, the incidence of NPM has increased, including GLM and PDM[3]. GLM was first defined by Kessler and Wolloch in 1972. The main features are noncaseating granuloma centered on the lobular unit of the breast, which are multifocal and of different sizes, with or without microabscess. PDM was first defined by Haagensen et al.[4]. In the lesions diagnosed as PDM, we can find that the mammary duct is highly dilated, and the capsule is filled with thick pink granular material; lymphocytes, plasma cells, and neutrophils infiltrated around the dilated duct.
The etiology of NPM is not fully understood, but alpha-1 antitrypsin deficiency, oral contraceptive usage, and hormonal disorders have been reported as presumptive causes [5]. Interestingly, hormones likely play a significant role in both PDM and GLM. In a study by Peters et al. [6], serum prolactin levels in 108 patients with NPM were determined before, during, and after treatment. They found that increased prolactin secretion caused mammary duct ectasia, and NPM may be a symptom of hyperprolactinemia. In the study of Radojković et al. [7], hyperprolactinemia was observed in the domain of mammary ductal secretory activity, leading to mammary secretion of lipid and protein materials and simultaneously increasing the number of ductal epithelial cells, ductal histiocytes, and “foam cells” macrophages. Similarly, Zhang et al. showed that high prolactin levels may be a trigger for PDM [8]. They also reported that five patients taking antipsychotic medications developed PDM, while psychotropic-associated PDM had not yet been reported. Destek et al [9]. reported that a patient diagnosed with idiopathic granulomatous mastitis initially presented with pituitary prolactinoma. Nikolaev et al [10]. reviewed four GLM cases with intracranial lesions, and suggested screening for pituitary tumors and evaluation of prolactin levels in the workup of GM patients without a recent history of lactation and pregnancy and no other identified etiology. In the pathology of these two cases, we found a number of dilated ducts, with thick secretion retention, lymphocyte infiltration, and chronic inflammation. Therefore, the pathogenesis of PDM and GLM in non-pregnant women may help us to understand the role of hyperprolactinemia in this disease.
Conclusions
NPM is a benign breast disease that differs from malignant breast tumors and is diagnosed through pathological methods. Although antibiotics, steroids, anti-tuberculosis drugs, and even surgery are used, the recurrence rate of NPM is still high, and there is a lack of standardized and unified treatment. At present, patients continue to take bromocriptine, and after 9 months of follow-up, the disease shows no tendency of relapse. This further demonstrates that hyperprolactinemia may promote NPM. In addition, we found that treating mastitis while reducing prolactin level is conducive to recovery. The current study from United States showed that idiopathic granulomatous mastitis is a self-limiting disease, that eventually resolves without resection. After diagnosis, medication is unnecessary, and operation can be limited to drainage procedures for fluid collection. Close observation, reassurance, and patient education should favored in the management of IGM [11]. Therefore, for patients diagnosed with NPM, we recommend exploring the possible etiological factors, and individualized treatment to reduce the recurrence rate.
Conflicts of Interest : There are no conflicts of interest to declare.
References
- Kaidi Zhang, Yong Yang, and Yongliang Gao. New Research Progress of Non-Puerperal Mastitis. Advances in Clinical Medicine. 2020; 10(05).
- Idiopathic granulomatous mastitis in Hispanic women - Indiana, 2006-2008. MMWR Morb Mortal Wkly Rep. 2009; 58(47): 1317- 21.
- Wang qi. Attention should be paid to the diagnosis and treatment of non-lactation mastitis [J]. Chinese journal of breast disease. 2013; 7(03): 154-156.
- Haagensen CD. Diseases of the female breast. Trans N Engl Obstet Gynecol Soc. 1956; 10: 141-56.
- Lin CH, et al. Idiopathic granulomatous mastitis associated with risperidone-induced hyperprolactinemia. Diagn Pathol, 2012; 7: 2.
- Peters F, W Schuth. Hyperprolactinemia and nonpuerperal mastitis (duct ectasia). Jama. 1989; 261(11): 1618-20.
- Radojković, D., et al. [Significance of hyperprolactinemia for cytomorphologic features of breast secretions]. Vojnosanit Pregl. 2010; 67(1): 42-7.
- Zhang Y., et al., Clinical characteristics, classification and surgical treatment of periductal mastitis. J Thorac Dis. 2018; 10(4): 2420- 2427.
- Destek S, et al., Pituitary Adenoma and Hyperprolactinemia Accompanied by Idiopathic Granulomatous Mastitis. Case Rep Endocrinol. 2017; 2017: 3974291.
- Nikolaev A, CN Blake, DL Carlson,.Association between Hyperprolactinemia and Granulomatous Mastitis. Breast J. 2016; 22(2): 224-31.
- Davis J., et al. Re-evaluating if observation continues to be the best management of idiopathic granulomatous mastitis. Surgery. 2019; 166(6):1176-1180.