
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Two cases of anomalous origin of left coronary artery from the pulmonary artery
Zhao Juan; Zou Chunbo*
Taizhou People’s Hospital, Taizhou, Jiangsu, 225300 China
*Corresponding Author: Zou Chunbo
Taizhou People’s Hospital, Taizhou, Jiangsu, 225300
China.
Email: shilz123@yeah.net
Received : Feb 01, 2022
Accepted : Feb 25, 2022
Published : Mar 04, 2022
Archived : www.jcimcr.org
Copyright : © Chunbo Z (2022).
Abstract
Coronary artery originating from pulmonary artery is a rare congenital vascular malformation, which generally presents corresponding clinical symptoms with the growth of patients’ age. Coronary CTA and angiography are important methods for diagnosis of this disease, and provide evidence for treatment strategies of patients.
Keywords: bicardiovascular malformations; coronary arteries; coronary cta.
Abbreviations: CTA: CT angiography; UCG: Ultrasound cardiogram; ECG: Electrocardiogram; ALCAPA: Anomalous origin of the left coronary artery from the pulmomaryartery.
Citation: Juan Z, Chunbo Z. Two cases of anomalous origin of left coronary artery from the pulmonary artery. J Clin Images Med Case Rep. 2022; 3(3): 1711.
Introduction
The origin of the left coronary artery from the pulmonary artery is rare in clinical practice, and the treatment experience is relatively lacking. With the development of science and technology, medical imaging is timely and more advanced, which is beneficial for us to more accurately observe the malformed blood vessels and disease changes in patients. Here, we introduce two cases
Case report
Case 1
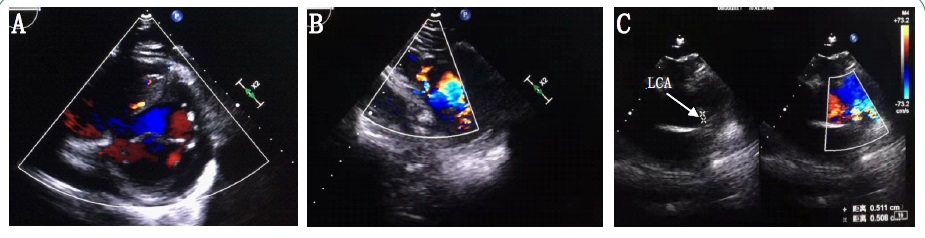
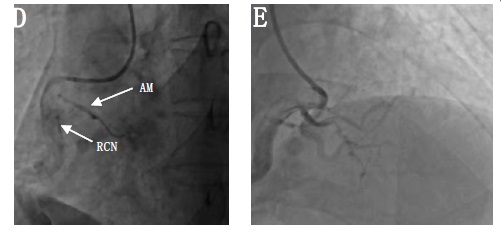
The patient, male, 53 years old, was admitted because of “chest tightness for 1 week”, BNP120 pg/ml. UCG showed abundant collateral blood flow in the ventricular septum (Figure 1A), and the left coronary artery was connected to the pulmonary artery. Blood flowed to the pulmonary artery in diastolic phase and pulmonary artery in systolic phase (Figure 1B,1C). Coronary angiography showed that the left coronary artery was absent and the right coronary artery was thick (Figure 1D,1E). Coronary CTA showed that the left coronary artery was connected to the pulmonary artery (Figure 1F). There were abundant collateral vessels in the interventricular septum (Figure 1G,H,I). The posterior interventricular branch of the right crown was connected with the end of the anterior descending branch of the left crown (Figure 1J). The right coronal conus branch and the anterior branch of the right ventricle are connected with the branches of the left anterior descending branch (Figure 1K). The left coronary artery was diagnosed as originating from the pulmonary artery. The patient’s symptoms spontaneously resolved after admission and surgical treatment was refused.
Case 2
A 46-year-old male patient was admitted to hospital due to “repeated chest tightness and asthma for 1 year and aggravation for 2 weeks after activities”. ECG suggested atrial fibrillation, BNP8667 pg/ml, UCG suggested abnormal coronary blood flow, left heart enlargement, left ventricular diastolic dysfunction (restrictive filling disorder), severe mitral regurgitation, moderate pulmonary hypertension, small amount of fluid in pericardium.
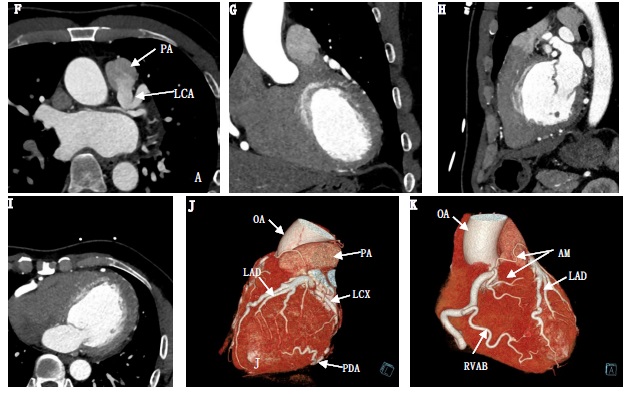
Coronary CTA indicated that the left coronary artery was connected with the pulmonary artery (Figure 2A,2B), and both the left and right coronary arteries were wide and malformed, with abundant collateral vessel formation between them (Figure 2C,D,E)

Coronary angiography: left coronary artery was absent and right coronary artery were wide malformation (Figure 2F,G), diagnosed as abnormal origin of coronary artery (left coronary artery originates from pulmonary artery), mitral valve replacement + left main trunk ligation + coronary artery bypass grafting were performed in our hospital.
Discussion
The Left Coronary Artery Originates from the Pulmonary Artery (ALCAPA) also known as bland-white-garland syndrome is a rare congenital abnormality first reported by Brooks in 1886 [1]. Approximately 1 in 300,000 live births [2]. The patient had no special discomfort in his childhood and young adulthood, but gradually presented with dyspnea, angina pectoris, syncope and other clinical symptoms as he grew older. Symptoms of ALCAPA are usually associated with myocardial ischemia. The lateral branch of the right coronary artery usually forms when pulmonary resistance drops and supplies blood to the left coronary artery to satisfy the oxygen consumption of the myocardium.
If the pulmonary artery perfusion pressure is reduced, blood flow in the left coronary artery will enter the pulmonary artery which called “steal blood” phenomenon, leading to ischemia and hypoxia in left ventricular. Large shunts from left to right often result in chronic ischemia, even with adequate collateral circulation.
In many cases, the anterolateral papillary muscle may contract due to scarring and calcification from chronic ischemia, a process that may lead to mitral regurgitation [3]. Mitral valve replacement may be considered in patients with severe mitral valve prolapse. The second patient had mitral regurgitation, which was considered to be related to papillary muscle ischemia. After mitral valve replacement + left main stem ligation + coronary artery bypass graft, the patient’s heart failure symptoms were significantly improved during a 3-year follow-up.
According to whether there is abundant collateral circulation between the left and right coronary arteries, the disease can be divided into infantile type and adult type. Because the pressure and oxygen saturation of the aorta and pulmonary artery in the fetus are equal, there are no obvious signs of disease during the fetus, and no collateral branches form during this time due to normal myocardial perfusion. However, after birth, pulmonary vascular resistance decreases and coronary artery theft occurs. The onset of symptoms depends on the number of collateral branches between the left and right coronary arteries and pulmonary artery pressure [4]. A review of ALCAPA patients showed that 66% of adult patients presented with angina, dyspnea, palpitations or fatigue. Ventricular arrhythmias, syncope, or sudden death occurred in 17% of patients, while 14% remained asymptomatic [5].
Surgery and percutaneous closure are the main treatment methods for these patients. Surgical treatment includes: (1) ligation of the left main artery and reconstruction of the left coronary artery system with a vein or internal mammary artery graft (2) direct or indirect reimplantation of the left aorta to the aorta via a pulmonary artery or internal iliac artery graft. Ligation of the abnormal artery with coronary artery bypass grafting is the preferred method in adults, and reimplantation of the left main coronary artery into the aorta is the most common technique in the pediatric population. The main treatment for minimally invasive percutaneous treatment was percutaneous ALCAPA closure with amplazee vascular occlude [6].
Imaging examination is crucial for the differential diagnosis of ALCAPA patients. Early diagnosis combined with necessary surgical treatment can significantly improve the prognosis of these patients.
Declarations
Acknowledgements: None.
Authors’ contributions: Z C B - acquisition of case and the preparation of the manuscript. Z J-planning and manuscript revision, interpretaion of results and making contributions to the conception of this study. All authors have read and approved this manuscript.
Funding: There was no funding for this study
Availability of cases and materials: All information are available from the corresponding author on reasonable request.
Ethics approval and consent to participate: This study has been granted an exemption from requiring ethics approval according to “The ethics committee of Taizhou People’s Hospital”.
Consent for publication: Obtained.
Competing interest: Z J and Z C B declare that they have no competing interests.
References
- Brooks HS. Two Cases of an Abnormal Coronary Artery of the Heart Arising from the Pulmonary Artery: With some Remarks upon the Effect of this Anomaly in producing Cirsoid Dilatation of the Vessels [J]. J AnatPhysiol. 1885; 20: 26-29.
- Paone G, Silverman N A. Anomalous origin of the left coronary artery from the pulmonary artery [J]. The Journal of Thoracic and Cardiovascular Surgery. 1994; 108: 1147.
- Lee Ac, Foster E, Yeghiazarians Y. Anomalous origin of the left coronary artery from the pulmonary artery: A case series and brief review [J]. Congenit Heart Dis. 2006; 1: 111-115.
- Yakut K, Tokel NK, Ozkan M, et al. Diagnosis and treatment of abnormal left coronary artery originating from the pulmonary artery: A single-center experience [J]. Anatol J Cardiol. 2019; 22: 325-331.
- Butt A, Amanullah MM, Amanullah MA, et al. Anomalous origin of the left coronary artery from the pulmonary artery: A surgical certainty [J]. Pak Med Assoc. 2020; 70: 561-564.
- Suzuki T, Ittleman FP, Gogo PB, Jr. Atypical presentation of anomalous origin of the left main coronary artery from the pulmonary artery [J]. Ann Thorac Surg. 2009; 88: 1339-1341.