
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Ulcerative colitis and cerebral venous thrombosis: A case report with literature review
Nesrine Kouki1*; Hanene Ben Rhouma1,2; Aida Rouissi1,2; Thouraya Ben Younes1,2; Hedia Klaa1,2; Ichraf Kraoua1,2; Ilhem Ben Youssef-Turki 1,2
1 Department of Child and Adolescent Neurology, Research laboratory LR18SP04, National Institute Mongi Ben Hmida of Neurology, Tunis, Tunisia.
2 University of Tunis El Manar, Faculty of Medicine of Tunis, Tunis 1007, Tunisia.
*Corresponding Author: Nesrine Kouki
Department of Child and Adolescent Neurology,
Research laboratory LR18SP04, National Institute
Mongi Ben Hmida of Neurology, Tunis, Tunisia.
Email: nesrine_kouki@yahoo.com
Received : Feb 01, 2022
Accepted : Feb 28, 2022
Published : Mar 07, 2022
Archived : www.jcimcr.org
Copyright : © Kouki N (2022).
Abstract
Background: Cerebral Venous Thrombosis is a rare complication of Inflammatory Bowel Disease and the pathogenesis underlying its incidence remains enigmatic.
Methods: We present a case of a child with a history of ulcerative colitis complicated with Cerebral venous thrombosis, and through the search engine ‘Pubmed’ we performed literature review to select similar cases in Pediatric population.
Results: In our case, Cerebral Venous Thrombosis was revealed by intense sharp headache just few days after a severe relapse under high oral doses of steroids and sulfasalazine. A cerebral Magnetic Resonance Imaging and Magnetic Resonance Angiography (MRA) showed an extended thrombosis complicated with cerebral infarction and hemorrhage.
The literature review showed that most Cerebral Venous Thrombosis came during or few months after a severe relapse incriminating a prothrombotic state secondary to systemic inflammation. Undergoing drugs intake was absent almost in half cases. Radiological findings supported the association with enlarged cerebral thrombosis.
Conclusion: Inflammatory Bowel Disease patients are associated with higher risk of thromboembolic complications. Early recognition and onset of the appropriate treatment prevent progression and complications which may be lethal.
Keywords: cerebral venous thrombosis; ulcerative colitis; headache; children.
Abbreviations: CVT: Cerebral Venous Thrombosis; IBD: Inflammatory Bowel Disorders; MRA: Magnetic Resonance Angiography; NR: Normal Range; NM: Not Mentioned; SSS: Superior Sagittal Sinus; UC: Ulcerative Colitis; VTE: Venous Thromboembolism; INR: International Normalized Ratio.
Citation: Kouki N, Rhouma HB, Rouissi A, Younes TB, Klaa H, et al. Ulcerative colitis and cerebralvenous thrombosis: A case report with literature review. J Clin Images Med Case Rep. 2022; 3(3): 1715.
Introduction
Cerebral venous thrombosis is a rare but a life threatening complication of inflammatory Bowel disease notably in ulcerative colitis.
Patients could suffer of this complication during or after a relapse of the disease, either under adjusted treatment or without any medications, the pathogenesis underlying its incidence remains enigmatic, therefore primary prevention is a laborious task for the physicians. Clinical manifestations of CVT are variable and include headaches, vomiting, focal neurologic deficit, and decreased level of consciousness. Here, we describe the atypical clinical presentation and treatment of a young man with CVT associated with UC.
Case report
A 16 year-old teenager born from a non-consanguineous marriage had a family history of type 1 diabetes in the sister. He had no significant antenatal or perinatal history. Psychomotor development was normal. He had no particular health complaints until 2020. At the age of 15, he started suffering from prolonged bloody stools. After biological and endoscopic explorations and based on the findings of intestinal tissue biopsy, the diagnosis of ulcerative colitis was made on January 2021 and the patient was put under an anti inflammatory combination of oral and rectal suppository treatment. The clinical remission was short and the patient was admitted in gastro-intestinal department on February 2021 for a severe relapse. The evolution was favorable under intravenous corticosteroids intake. The patient was discharged 3 weeks later with a medical prescription of oral high doses of steroids and oral sulfasalazine.
One week later, he was referred to the neurological emergency department for acute severe and sharp headache that started 3 days ago. Headache was constructive, localized on the left hemicranial side, and preventing the sleep, with no respond to paracetamol intake. He had no blurred vision or vomiting.
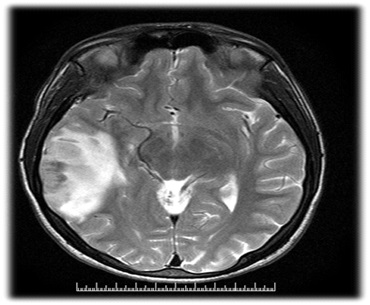
The neurological examination showed no abnormalities. A cerebral Magnetic Resonance Imaging (MRI) and Magnetic Resonance Angiography (MRA) were performed and showed an extended thrombosis of the right sigmoid and transverse sinuses reaching the internal jugular vein complicated with a cerebral infarction of the right temporoparietal lobes with hemorrhage (Figure 1).
Laboratory findings showed: An elevated white blood cells count at 20,000/mm3 (Normal Range (NR): 4.000-10.000/mm3 ), a hypochromic Anemia at 7 g/dl (NR: 12.5-17.5 g/dl), a normal platelets rate, CRP was normal, liver and renal function were within normal limits.
He was admitted in pediatric neurological department. The patient had prothrombotic assessment for antithrombin III, protein S, protein C deficiencies and anti phospholipid antibody syndrome were normal, plasma homocysteine level was normal.
Anticoagulation treatment was initiated with intravenous unfractionated heparin infusion, and oral acenocoumarol was introduced 5 days after reaching an activated Partial thromboplastin time of 70 seconds.
During hospitalization, the evolution was favorable, the patient didn’t develop any new symptoms and headache gradually improved.
He was discharged 2 Weeks later after a total recovery with an oral anticoagulation treatment based on acenocoumarol one tablet three times daily with an INR in the therapeutic range.
Discussion
Inflammatory Bowel Disease (IBD) has intestinal and extra intestinal manifestations which can affect central nervous system. In fact, IBD patients are at a 2 to 3 -fold higher risk of developing a Venous Thromboembolism (VTE) compared to the general population [1].
A precise incidence is not yet well described, but CVT seems to be more common in ulcerative colitis than in Crohn’s disease [2].
The presence of headache or acute worsening of neurological status in a patient with IBD should alert clinicians about the possibility of CVT.
Only ten pediatric cases of CVT in ulcerative colitis patients were described in literature all summarized in Table 1.
Table 1: Ulcerative colitis and CVT in pediatric population reported in litterature
Investigations |
Patient 1 |
Patient 2 |
Patient 3 |
Patient 4 |
Patient 5 |
Patient6 |
Patient 7 |
Patient 8 |
Patient 9 |
Patient 10 |
Our case |
Age(years) |
12 |
17 |
12 |
10 |
11 |
18 |
16 |
18 |
14 |
14 |
16 |
Gender |
female |
male |
male |
male |
Female |
male |
female |
male |
female |
male |
male |
Time between IBD diagnosis and CVT |
Diagnosed with CVT |
1.5 year |
4 years |
3 years |
3 years |
1 years |
1.5 years |
5.5 years |
Diagnosed with CVT |
Diagnosed with CVT |
3months |
Date of last relapse |
Concomittant to CVT |
3 weeks before |
Concomittant to CVT |
Concomittant to CVT |
Concomittant to CVT |
Concomittant to CVT |
Concomittant to CVT |
1 month before |
Concomittant to CVT |
Concomittant to CVT |
1 month before |
Severity of the last relapse |
severe |
moderate |
NM |
NM |
NM |
moderate |
severe |
severe |
severe |
severe |
severe |
Undergoing treatment |
NM |
No |
NM |
NM |
NM |
steroids intake |
No |
High doses of steroids +sulfasalazine |
No |
No |
High doses of steroids +sulfasalazine |
Clinical presentation |
left-sided hemiparesis + numbness + intermittent convulsion |
Acute Headache |
Acute Headache |
Acute Headache |
Acute headache |
Acute headache |
Acute headache+ |
Acute headache |
Paresthesia and partial motor deficit of the left lower limb |
Headache+ hemiparesis + |
Acute headache |
Biological abnormalities |
Hyperleukocytosis+moderate anemia |
low protein S levels |
NM |
NM |
NM |
NM |
mild thrombocytosis +anemia+high CRP |
anemia |
Hyperleukocytosis+ Hypertransaminasemia+high CRP |
Hyperleukocytosis + anemia |
Hyperleukocytosis + anemia |
Immunological tests |
negative |
negative |
negative |
NM |
NM |
negative |
negative |
negative |
negative |
negative |
negative |
Radiological findings |
VT of the SSS with secondary hemorrhage and infarction in frontal and temporal lobes |
VT of the right transverse and sigmoid sinuses |
NM |
NM |
NM |
VT of the left lateral sinus |
left lateral and sigmoid sinuses thrombosis with left temporal infarction |
VT of the transverse sinus |
VT of the sagittal sinus infarction |
VT of the sigmoid and lateral sinuses extending to the internal jugular vein + hemorragic infarction |
extended thrombosis of the right sigmoid and transverse sinuses reaching the internal jugular vein complicated with a cerebral infarction of the right temporoparietal lobes with hemorrhage |
Evolution |
complete recovery |
complete recovery |
complete recovery |
Coma and Death |
Death |
complete recovery |
complete recovery |
complete recovery |
complete recovery |
complete recovery |
Complete recovery |
reference |
Medecine , 2020 [10] |
Brain & Development (2011) [11] |
Journal of Digestive Diseases 2015 [12] |
Revue de la medecine interne 2006[13] |
Acta Gastro-enteroogica Belgica,2007[14] |
World journal of Gastroenterology ,2008[15] |
Pediatrics, 2013 [16] |
Journal of pediatric gastroenterologyand nutrition ,1989 [17] |
|
||
Abbreviations : NM :not mentionned / VT: venous thrombosis/ SSS: superior sagittal sinus ;
In our case, cerebral venous thrombosis was revealed by intense isolated headache and consistent with the findings in the reviewed pediatric cases (Table 1). Indeed, based on the International classification of headache disorders 3rd edition, in CVT headache is by far the most frequent symptom and has no specific characteristics but most often, is diffuse and severe [3,4].
The pathogenesis of CVT relies on interrelated Factors. IBD is known to cause an effective systemic inflammation considered as a prothrombotic state [5] which is in its highest level during relapses explaining the short delay between relapse and clinical manifestation in the case we report. Aside from inflammation, other factors such as anemia, thrombophilia and corticoids intake are incriminated.
Screening for prothrombotic conditions is systematic considering its possible association with IBD and its contribution in determining the duration of oral anticoagulation.
Radiological findings revealed that the involvement of multiple sinuses and extensive venous clot were more associated with hemorrhagic infarction than those with nonhemorrhagic lesions (Table 1). Patients with haemorrhagic infarction usually have more disability after 3 months of evolution compared to those with non haemorrhagic lesions [6], luckily our patient only suffered from headache which improved rapidly after the onset of treatment.
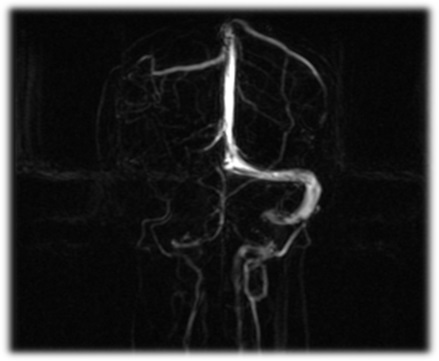
The prothrombotic state in CVT is thought to explain the enlarged thrombosis [6], explaining the cerebral MRI results found in our patient with the clot reaching the internal jugular vein. (Figure 2).
In IBD, the underwent therapy interferes with the pathogenesis of CVT. Indeed, Corticosteroids as previously mentioned may induce a hypercoagulability state by activating the coagulation Factors FVII, VIII and XI and by blocking the anticoagulation mechanisms [7]. This adverse effect is described especially with high doses [8] which was the case of our patient. On the other hand, Aminosalicyclates such as Sulfasalazine may inhibit spontaneous and thrombin-induced platelet activation which has been thought to reduce VTE risks [9].
The current practice in the treatment of CVT in patient with IBD is similar to patients without IBD, but the duration may differ depending on the results of etiological investigation [7].
The screening of an associated prothrombotic disease was negative in our patient.
Our case represents an unusual complication of ulcerative colitis. Indeed, IBD is recognized as a risk factor for VTE. The underlying mechanisms are Interrelated but not well-elucidated. Acute onset of Neurological symptoms in IBD patients, should alarm clinicians to consider TVC diagnosis and start an early treatment minimizing complications that may be lethal.
Declarations
Funding: No funding was received towards this work.
Competing interests: The authors report no competing interests.
Ethics approval: Not applicable.
Informed consent: The patient authorized the writing and publication of this case report.
Author participations: -Nesrine kouki; Hanene Ben Rhouma, Aida Rouissi, Thouraya Ben Younes, Hedia Klaa, Ichraf Kraoua and Ilhem Ben Youssef Turki participated in taking care of the patient and the bibliography RESEARCH. -Nesrine kouki and Hanene Ben Rhouma participated in the design and writing the final manuscript.
References
- Grainge, Matthew J, West Joe, Et card, timothy R. Venous thromboembolism during active disease and remission in inflammatory bowel disease: a cohort study. The Lancet. 2010; 375: 657- 663.
- Goh IY, Saric S , Leschke P, McFarlane M, Jha PK, et al. Thromboembolism in active ulcerative colitis. BMJ Case Reports. 2017; 2017 p. bcr-2016-218608.
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018; 38: 1–211.
- Katsanos AH, Katsanos KH, Kosmidou MS, Giannopoulos AP, Kyritsis EV, et al. Tsianosl. Cerebral sinus venous thrombosis in inflammatory bowel diseases. QJM: An International Journal of Medicine. 2013; 106: 401-413.
- Owczarek D, Cibor D, Głowacki MK, Tomasz Rodacki , Tomasz Mach Inflammatory bowel disease: Epidemiology, pathology and risk factors for hypercoagulability. World Journal of Gastroenterology. 2014; 20: 53.
- Kumral E, Polat F, Uzunköprü C, C Callı, Ö Kitiş. The clinical spectrum of intracerebral hematoma, hemorrhagic infarct, nonhemorrhagic infarct, and non-lesional venous stroke in patients with cerebral sinus-venous thrombosis. European Journal of Neurology. 2011; 19: 537–543.
- Zezos P, Kouklakis G, Saibil F. Inflammatory bowel disease and thromboembolism. World Journal of Gastroenterology. 2014; 20: 13863.
- Wei L, MacDonald TM, Walker BR. Taking glucocorticoids by prescription is associated with subsequent cardiovascular disease. Annals of internal medicine. 2004; 141: 764-770.
- Cheng K, Faye AS. Venous thromboembolism in inflammatory bowel disease. World journal of gastroenterology. 2020; 26: 1231.
- Liu Y, Ren D, Zhou Q, Gao L. Cerebral sinovenous thrombosis in a child with ulcerative colitis: A case report. Medicine (Baltimore). 2020; 99.
- Maria Diakou M, Kostadima V, Giannopoulos S, Zikou AK, Argyropoulou MI, Kyritsis AP, et al. Cerebral venous thrombosis in an adolescent with ulcerative colitis. Brain and Development. 2011; 33: 49-51.
- DeFilippis EM, Barfield E, Leifer D, Steinlauf A, Bosworth BA, et al. Cerebral venous thrombosis in inflammatory bowel disease. Journal of digestive diseases. 2015; 16: 104-108.
- Béchade D, Desramé J, Sallansonnet Froment M, Taillia H, Algayres JP, et al. Thrombose veineuse cérébrale et rectocolite hémorragique. La Revue de médecine interne. 2006; 27: 958-961.
- Ennaifer R, Moussa A, Mouelhi L. Cerebral venous sinus thrombosis as presenting feature of ulcerative colitis. Acta gastro-enterologica Belgica. 2009; 72: 350-353.
- Thorsteinsson GS, Magnussson M, Hallberg LM, Wahlgren NG, Lindgren F, et al. Cerebral venous thrombosis and heparininduced thrombocytopenia in an 18-year old male with severe ulcerative colitis. World Journal of Gastroenterology. 2008; 14: 4576.
- Maggi U, Rossi G, Avesani EC. Thrombotic Storm in a Teenager with Previously Undiagnosed Ulcerative Colitis. PEDIATRICS. 2013; 131: e1288–e1291.
- Markowitz RL, Ment LR, Gryboski JD. Cerebral Thromboembolic Disease in Pediatric and Adult Inflammatory Bowel Disease. Journal of Pediatric Gastroenterology and Nutrition. 1989; 8: 413–420.