
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
An uncommon association of L-asparaginase with gastrointestinal vascular congestion
Shi Hui Clarice Choong1*; Winnie ZY Teo1,2; Eng Soo Yap1,3
1 Department of Haematology-Oncology, National University Cancer Institute Singapore (NCIS), National University Health System, Singapore.
2 Fast Program, Alexandra Hospital, National University Health System, Singapore.
3 Department of Laboratory Medicine, National University Hospital, National University Health System, Singapore.
*Corresponding Author: Shi Hui Clarice Choong
Department of Haematology-Oncology, Tower
block, level 7, 1E Kent Ridge Rd, Singapore 119228.
Email: clarice_choong@nuhs.edu.sg
Received : Feb 03, 2022
Accepted : Mar 01, 2022
Published : Mar 08, 2022
Archived : www.jcimcr.org
Copyright : © Choong CSH (2022).
Abstract
A 71-year-old Chinese female was admitted with nasal symptoms and biopsy of her right nasal mass confirmed extra-nodal Natural Killer/T (NK/T) cell lymphoma. She was commenced on combination chemotherapy regime consisting of Prednisolone, Vincristine and L-asparaginase. Six days after initiation of chemotherapy, she developed an acute onset of generalized 2 abdominal distension with large amount of ascites. A Computed Tomography scan of her abdomen and pelvis showed stomach and proximal small bowel oedema and non-specific hyper densities within her duodenum. A pushed enteroscopy and colonoscopy subsequently showed a highly oedematous gastrointestinal tract, making it extremely challenging to scope. Multiple biopsies of her stomach corpus and fundus were acquired which revealed vascular congestion of the gastric body-type mucosa, with no malignancy involved, demonstrating a rare association of gastrointestinal vascular congestion with L-Asparaginase.
Keywords: L-Asparaginase; extra nodal nk/t cell lymphoma; vascular congestion; hypercoagulable state.
Citation: Choong CSH, Teo WZY, Yap ES. An uncommon association of L-Asparaginase with gastrointestinal vascular congestion. J Clin Images Med Case Rep. 2022; 3(3): 1720.
Introduction
L-asparaginase has been the main component of the treatment for patients with acute lymphoblastic leukaemia since its introduction to paediatric chemotherapy protocol in the 1960s. With its introduction, the overall survival rates in the younger population have steadily improved to estimated 90% [1]. With its efficacy, it has been used in treatment protocols for selected cases of extra-nodal NK/T cell lymphomas [2].
L-asparaginase is mainly an enzyme which breaks down the amino acid known as Lasparagine. The latter is an endogenous amino acid that is essential for the activities of neoplastic cells. With the reduction of L-asparagine in the plasma, this prevents further RNA and DNA synthesis and eventually leads to apoptosis of the neoplastic cells [3].
However, several toxicities related to L-asparaginase chemotherapy such as hypersensitivity, acute pancreatitis, liver dysfunction, and thrombotic issues have been reported [4]. Regarding the thrombotic incidence among patients with acute lymphoblastic leukaemia, it has been demonstrated to have a wide range from 1% to 36%, depending on the various clinical factors 3 such as age, patient population, treatment protocol, etc. Majority of the thrombosis sites are documented to be located at the upper extremity central catheter related, lower extremities and central nervous system related thrombosis [5].
However, few cases of L-asparaginase induced gastrointestinal vascular congestion have been described. Therefore, we present a case of an elderly patient with extra-nodal Natural Killer/T (NK/T) cell lymphoma on L-asparaginase based chemotherapy who presented with gastrointestinal vascular congestion.
Case report
A 71 years old Chinese female was admitted for investigation of a right nasal mass. She had a medical history of hypertension, bilateral osteoarthritis of the knees and previous cholecystectomy for gallstones. A biopsy of the nasal mass confirmed the diagnosis of an extranodal Natural killer/T (NK/T) cell lymphoma and she was commenced on a combination chemotherapy regime consisting of Prednisolone, Vincristine and L-asparaginase.
Six days after initiation of chemotherapy, she developed sudden onset of abdominal pain, distension and an episode of haematochezia. On examination, she was pallid, mildly tachypnoeic with generalized oedema. She had generalized abdominal distension with large amount of ascites without signs of peritonism. Her vitals were otherwise stable. A digital rectal examination and proctoscopy did not reveal an obvious source of bleeding.
The abnormalities in her laboratory tests included: Total white cell count- 5.22 X 109 /L; Haemoglobin- 12.2 g/dL; Platelets-123 X 109 /L; Prolonged prothrombin time and partial thromboplastin time at 28.4 seconds and 49.0 seconds respectively; Fibrinogen-1.89 g/L; Low albumin- 20 g/L and elevated lactate-3.4 mmol/L.
A Computed Tomography scan of her abdomen and pelvis showed stomach and proximal small bowel oedema (Figure 1A) and nonspecific hyper densities within the second part of the duodenum. (Figure 1B).


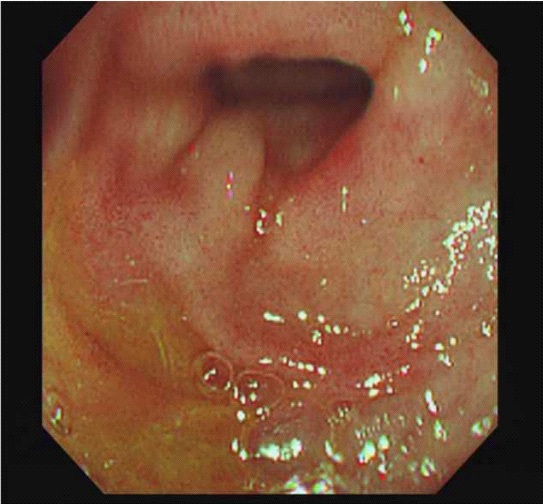
A pushed enteroscopy and colonoscopy indicated that her stomach was arduous to insufflate fully and there was much difficulty in retro-flexing the endoscope. The gastric mucosa appeared thickened and irregular (Figure 1C). It was also noted that her gastrointestinal tract was equitably oedematous, making her scopes a challenge.
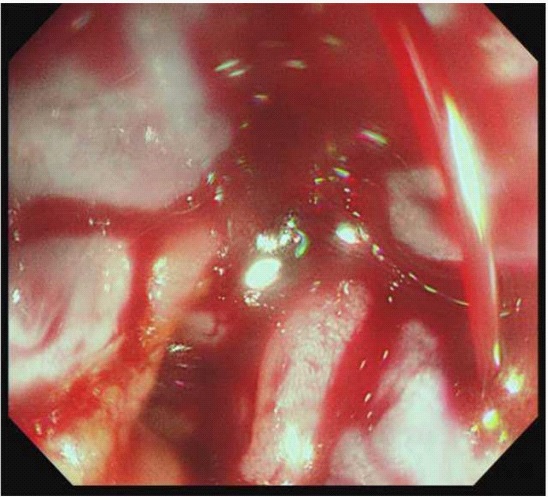
Colonoscopy revealed massively bleeding haemorrhoids for which stitching and sclerodermic injections had to be performed to secure haemostasis (Figure 1D). Multiple biopsies of her stomach corpus and fundus were obtained. Histopathology revealed superficial vascular congestion of the gastric bodytype mucosa. There was no significant inflammation, intestinal metaplasia, dysplasia or malignancy noted. There was no Helicobacter pylori infection.
Discussion
L-asparaginase chemotherapy has been widely used for the treatment of acute lymphoblastic leukaemia [6] and in selected cases of extra-nodal NK/T cell lymphoma, nasal type. Lasparaginase hydrolyses asparagine to aspartic acid and ammonia. This results in decreased protein synthesis, followed by cellular apoptosis, leading to either increased haemorrhagic or thromboembolic events [7]. Examples of which include hypofibrinogenemia, hepatic toxicity, deep vein thrombosis [8], acute pancreatitis [9], and cerebral sino-venous thrombosis in children [10].
However, reports of L-asparaginase resulting in gastrointestinal vascular congestion are not well reported to date.
This case report showed that depression of the clotting factors from L-asparaginase had resulted in vascular congestion of the patient’s gastrointestinal tract, resulting in symptoms of abdominal distension and oedema.
In addition, depletion of clotting factors also precipitated and worsened the patient’s haemorrhoids with consequential persistent per rectal bleed.
Further studies in future can hopefully look out earlier for similar association of venous congestion with L-asparaginase and mitigate the consequences.
References
- Egler, Rachel A, et al. L-asparaginase in the treatment of patients with acute lymphoblastic leukemia. Journal of pharmacology & pharmacotherapeutics. 2016; 7: 62-71.
- Kwong YL, Kim WS, Lim ST, et al. SMILE for natural killer/T-cell lymphoma: Analysis of safety and efficacy from the Asia Lymphoma Study Group. Blood. 2012; 120: 2973-2980.
- Piatkowska-Jakubas B, Krawczyk-Kuliś M, Giebel S, et al. Polish Adult Leukemia Group. Use of L-asparaginase in acute lymphoblastic leukemia: Recommendations of the Polish Adult Leukemia Group. Pol Arch Med Wewn. 2008; 118: 664-669.
- Hijiya N, van der Sluis IM. Asparaginase-associated toxicity in children with acute lymphoblastic leukemia. Leuk Lymphoma. 2016; 57: 748-757.
- Goyal, Gaurav, Vijaya Raj Bhatt. “L-asparaginase and venous thromboembolism in acute lymphocytic leukemia.” Future oncology (London, England). 2015; 11: 2459-2470
- Narta U.K, Kanwar S.S, Azmi W. Pharmacological and clinical evaluation of Lasparaginase in the treatment of leukemia. Crit Rev Oncol Hematol. 2007; 61: 208–221.
- Castaman G, Rodeghiero F, Dini E, et al. Thrombotic complications during Lasparaginase treatment for acute lymphocytic leukemia. Haematologica. 1990; 75: 567– 569.
- Beinart G, Damon L. Thrombosis associated with L-asparaginase therapy and low fibrinogen levels in adult acute lymphoblastic leukemia. Am. J. Hematol. 2004; 77: 331–335.
- Ho DHW, Yap HY, Brown N, et al. Clinical pharmacology of intramuscularly administered L-asparaginase, J. Clin. Pharmacol. 1981; 27: 72-78.
- Caruso V, Iacoviello L, Castelnuovo A, et al. Thrombotic complications in childhood acute lymphoblastic leukemia: A metaanalysis of 17 prospective studies comprising 1752 pediatric patients. Blood. 2006; 108: 2216–2222.