
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Isolated tricuspid valve disease in antiphospholipid syndrome
Ron Edri1; Yuval Ishay2; Limor Rubin3; Fadi Kharouf1,4*
1 Department of Medicine, Hadassah Medical Center and Faculty of Medicine, Hebrew University of Jerusalem, Israel.
2 Allergy and Clinical Immunology Unit, Hadassah Medical Center and Faculty of Medicine, Hebrew University of Jerusalem, Israel.
3 Institute of Gastroenterology and Hepatology, Hadassah Medical Center and Faculty of Medicine, Hebrew University of Jerusalem, Israel.
4 Rheumatology Unit, Hadassah Medical Center and Faculty of Medicine, Hebrew University of Jerusalem, Israel.
*Corresponding Author: Fadi Kharouf
Department of Medicine and the Rheumatology
Unit, Hadassah Medical Center and Faculty of Medicine, Hebrew University of Jerusalem, Israel.
Email: fadikharouf@hotmail.com
Received : Jan 20, 2022
Accepted : Mar 02, 2022
Published : Mar 09, 2022
Archived : www.jcimcr.org
Copyright : © Kharouf F (2022).
Abstract
We report the case of a 27-year-old male, presenting with dyspnea and chest pain. Radiographic and echocardiographic evaluations revealed bilateral segmental pulmonary embolism, left lower extremity deep vein thrombosis, and isolated tricuspid valve endocarditis. Microbiologic and serologic tests ruled out an infectious etiology and supported a diagnosis of nonbacterial thrombotic endocarditis as a manifestation of a newly diagnosed antiphospholipid syndrome. We discuss the clinical presentation, diagnostic evaluations, treatment, and clinical outcome.
Keywords: pulmonary embolism; tricuspid valve; nonbacterial thrombotic endocarditis; antiphospholipid syndrome.
Abbreviations: Caβ2GPI: Anti-beta-2-glycoprotein I; aPL: Antiphospholipid antibodies; APS: Antiphospholipid syndrome; CTA: Computed tomography angiography; COVID-19: Coronavirus disease 2019; DVT: Deep vein thrombosis; LLL: Left lower lobe; LSE: Liebman-Sacks endocarditis; NBTE: Non-bacterial thrombotic endocarditis; PCR: Polymerase chain reaction; PE: Pulmonary embolism; SARS-CoV-2: Severe acute respiratory syndrome-coronavirus-2; SLE: Systemic lupus erythematosus; TTE: Transthoracic echocardiography; TR: Tricuspid regurgitation;
Citation: Edri R, Ishay Y, Rubin L, Kharouf F. Isolated tricuspid valve disease in antiphospholipid syndrome. J Clin Images Med Case Rep. 2022; 3(3): 1724.
Introduction
Nonbacterial thrombotic endocarditis (NBTE) is characterized by non-infectious valvular vegetations consisting of fibrin and platelet deposits. It is associated with numerous diseases, including systemic lupus erythematosus (SLE), antiphospholipid syndrome (APS), advanced malignancy, and to a lesser extent sepsis and burns [1]. APS, an acquired autoimmune thrombophilia, is characterized by vascular thrombosis and/or obstetric morbidity along with persistently present antiphospholipid antibodies (aPL). The overall prevalence of APS has been estimated at 50 per 100,000 persons, with a female predominance [2]. NBTE is the main manifestation of cardiac APS, with the left-sided heart valves involved in virtually all cases. Isolated involvement of the tricuspid valve is exceedingly rare, observed mainly in young females [3]. Herein, we describe a unique case of APS, presenting as bilateral pulmonary embolism (PE), left lower extremity deep vein thrombosis (DVT), and isolated tricuspid NBTE.
Case presentation
A 27-year-old generally healthy male, presented to the emergency room with a two-week history of exertional dyspnea, pleuritic chest pain, and left calf pain. He denied fever, recent illness, abdominal symptoms, and any history of trauma or immobilization. The patient denied tobacco, alcohol or illicit drugs use and led a sedentary lifestyle. Family history was notable for a mother with obstetric APS. Upon admission, he was hemodynamically stable but tachycardic (103 beats/min) and tachypneic (25 breaths/min), with no fever. His oxygen saturation was 92% on room air. He appeared weak and dyspneic. Physical exam revealed reduced air entry to the lung bases bilaterally and crackles over the left lower lobe (LLL). Lower limb examination was unremarkable.
His labs were notable for mild thrombocytopenia (100,000/ mm3 , reference: 150,000-450,000/mm3 ), high C-reactive protein (10.9 mg/dL, reference: < 0.5 mg/dL), and prolonged partial thromboplastin time (85 seconds, reference: 22.4-36.3 seconds). Cardiac enzymes were normal. The electrocardiogram was normal apart from sinus tachycardia. Nasopharyngeal swabs for SARS-CoV-2 were negative. Chest X-ray showed a consolidation in the LLL and chest computed tomography angiography showed bilateral segmental PE and a LLL infiltrate. After obtaining blood cultures, treatment with low molecular weight heparin (LMWH) and ceftriaxone was initiated, and the patient was admitted to the internal medicine ward. The following day, transthoracic echocardiography (TTE) revealed a 10X10 mm mass on the tricuspid valve (Figure 1A), accompanied by severe tricuspid regurgitation (Figure 1B) and mild pulmonary hypertension. There were no signs of right ventricular strain. Work-up for infective endocarditis was initiated, including additional sets of blood cultures, bacterial serologies (Brucella, Coxiella burnetii and Treponema pallidum), rheumatoid factor and complement levels, as well as ophthalmologic evaluation. All tests were normal. His calf pain was assessed via leg ultrasound, showing an extensive left leg DVT. Lacking evidence for infection, the patient appeared to suffer unprovoked thrombotic events, and a directed workup was initiated. aPL serologies showed elevated titers of anti-cardiolipin and anti-β2-glycoprotein I IgM and IgG antibodies, with positive lupus anticoagulant (Table 1). In light of these findings, a diagnosis of APS was strongly considered, with the tricuspid vegetation presumed to represent NBTE/ Libman-Sacks endocarditis (LSE). Exhaustive history-taking, immunoserologies for antinuclear antibodies and SARS-CoV-2 antibodies were normal, precluding alternative diagnoses such as SLE and COVID-19. The final diagnosis was “triple-positive” primary APS, complicated by NBTE/LSE and DVT/PE. Treatment with enoxaparin was continued, and patient was discharged following clinical improvement. Repeat TTE examinations confirmed the stability of the finding and no involvement of other valves. Repeat aPL serologies performed 3 months following the index event were again positive, confirming the diagnosis.
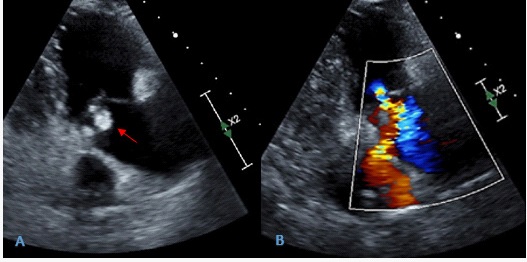
Table 1: Lab results for antiphospholipid antibodies.
|
Results |
Reference range |
Anti-cardiolipin IgM (U/mL) |
18.1 |
<7 |
Anti-cardiolipin IgG (U/mL) |
38.5 |
<10 |
Anti-β2GPI IgM (U/mL) |
5.2 |
<5 |
Anti- β2GPI IgG (U/mL) |
53.6 |
<5 |
Circulating anticoagulant Ratio |
4.13 |
<1.4 |
Diluted Russell Viper Venom Time Ratio |
2.68 |
<1.35 |
Β2GPI: beta-2-glycoprotein I
Discussion
We describe a unique case of tricuspid valve NBTE as the presenting manifestation of APS in a young healthy male. DVT and PE further complicated his APS in our case. Cardiac involvement in APS is common, with up to one third of the patients presenting with valvular abnormalities. Additional cardiovascular manifestations my include accelerated atherosclerosis, myocardial dysfunction, and pulmonary thromboembolism [3]. Valvular manifestations are variable, ranging from clinically silent disease to severe, symptomatic valvular dysfunction requiring surgical intervention. Clinically significant disease is reported in 3-5% of the patients [3]. The exact mechanism of APS-related thrombosis is not fully understood, with evidence suggesting involvement of prothrombotic, proinflammatory, and proangiogenic pathways. A key factor in the pathogenesis is the binding of β-2 glycoprotein I (β2GPI) to negatively charged phospholipids on the surface of endothelial cells, causing a conformational change and exposing an immunogenic β2GPI domain to the immune system. Ensuing inflammation drives localized recruitment of inflammatory cells and activation of the coagulation cascade, both pro-thrombotic events. These ongoing processes constitute the “first hit”. The “second hit”, required for overt clinical thrombosis, is likely a secondary prothrombotic event (e.g. infection) provoking thrombosis in the predisposed patient. Evidence suggests this thrombosis is a product of the action of monocytes, platelets, neutrophils, and complement proteins. This process is probably more pronounced in areas with turbulent blood flow, such as left-sided heart valves [2-4]. The tricuspid valve is rarely involved, and its involvement may be associated with DVT, PE and pulmonary hypertension [5]. Patients positive for all aPL tests, often termed “tripe positive”, are at a higher risk of thrombosis [2-4]. Conceivably, these patients may be prone to right-sided vegetations, less dependent on a conducive, turbulent environment to form clots.
Echocardiography is the cardinal tool for the diagnosis of valvular lesions in APS. Sonographic characteristics may allow to distinguish APS involvement from infective endocarditis, such as the lack of abscess formation or valve destruction, and the presence of leaflet thickening [3]. In non-obstetric APS, indefinite anticoagulation with vitamin K antagonists, such as warfarin, is the cornerstone of therapy. Other therapeutic options include LMWH and unfractionated heparin. When valvular involvement persists despite anticoagulation, indications for surgical intervention are the same as those for infective endocarditis, and rarely required [3,6]. Immunosuppressive therapy has not shown benefit in these patients. In fact, corticosteroids have been demonstrated to lead to valvular scarring, deformities, and dysfunction [4]. Optimal follow-up has not been defined, and must be tailored to the individual patient. Monitoring for complications of NBTE (e.g. embolization), and complications of therapy (e.g. hemorrhage) are essential. Periodic assessment of the vegetations is usually done [7].
Conclusions
Our case has several unique aspects. It describes a rare presentation of isolated tricuspid valve NBTE in APS; only scarce similar reports appear in literature. It underlines the need for pro-thrombotic assessment during the index presentation in appropriate patients, and may allow to correctly diagnose these patients, who may otherwise be labeled as suffering from infection-related thrombosis only. It again emphasizes the extreme thrombogenicity of triple positive APS.
Declarations
Statement of ethics: The patient has given his informed consent to publish his case (including publication of images).
Conflict of interest statement: The authors have no conflict of interests to declare.
Funding sources: No funding was received.
Data availability statement: Data can be made available through contact with the corresponding author Fadi Kharouf, through fadikharouf@hotmail.com.
Author contributions: The four authors have contributed to the care of the patient and to the writing of the manuscript.
References
- Asopa S, Patel A, Khan OA, Sharma R, Ohri SK. Non-bacterial thrombotic endocarditis. Eur J Cardiothorac Surg. 2007; 32: 696- 701. 10.1016/j.ejcts.2007.07.029
- Cohen H, Cuadrado MJ, Erkan D, Duarte-Garcia A, Isenberg DA, Knight JS, et al. 16th International Congress on Antiphospholipid Antibodies Task Force Report on Antiphospholipid Syndrome Treatment Trends. Lupus. 2020; 29: 1571-1593. 10.1177/0961203320950461
- Denas G, Jose SP, Bracco A, Zoppellaro G, Pengo V. Antiphospholipid syndrome and the heart: a case series and literature review. Autoimmun Rev. 2015; 14: 214-22. 10.1016/j.autrev.2014.11.003
- Hojnik M, George J, Ziporen L, Shoenfeld Y. Heart valve involvement (Libman-Sacks endocarditis) in the antiphospholipid syndrome. Circulation. 1996; 15: 1579-87. 10.1161/01.cir.93.8.1579
- Roldan CA. Valvular and coronary heart disease in systemic inflammatory diseases: Systemic Disorders in heart disease. Heart. 2008; 94: 1089-101. 10.1136/hrt.2007.132787
- Rabinstein AA, Giovanelli C, Romano JG, Koch S, Forteza AM, Ricci M. Surgical treatment of nonbacterial thrombotic endocarditis presenting with stroke. J Neurol. 2005; 252: 352-5. 10.1007/ s00415-005-0660-z
- Roldan CA, Sibbitt WJ, Qualls CR, Jung RE, Greene ER, Gasparovic CM, et al. Libman-Sacks endocarditis and embolic cerebrovascular disease. JACC Cardiovasc Imaging. 2013; 6: 973-83. 10.1016/j.jcmg.2013.04.012