
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A rare coexistence of ankylosing spondylitis and SCD: Pitfalls and challenges during THA
Vikram I Shah1; Javahir A Pachore2*; Jayesh Patil3; Darshan Rajani4; Gautam M Shetty5,6
1 Founder and Chairman, Shalby Hospital, Ahmedabad, India.
2 Director of Hip Surgery and Head of Department of Orthopaedics, Shalby Hospital, Ahmedabad, India.
3 Senior Consultant Joint Replacement, Shalby Hospital, Ahmedabad, India
4 Resident, Department of Orthopaedics, Shalby Hospital, Ahmedabad, India.
5 Consultant Orthopaedic Surgeon, Knee and Orthopaedic Clinic, Mumbai, India
6 Head of Research, AIMD Research, India.
*Corresponding Author: Javahir A Pachore
Shalby Multi-speciality Hospital, Sarkhej-Gandhinagar Highway, Opposite Karnavati Club, Ramdev
Nagar, Ahmedabad 380015, Gujarat, India.
Email: pachorejavahir@gmail.com;
japachore@rediffmail.com
Received : Feb 07, 2022
Accepted : Mar 04, 2022
Published : Mar 11, 2022
Archived : www.jcimcr.org
Copyright : © Pachore JA (2022).
Abstract
The co-existence of Ankylosing Spondylitis (AS) and Sickle Cell Disease (SCD) is extremely rare, and the case of such a patient undergoing Total Hip Arthroplasty (THA) has never been reported. We present a case report of a 39-year-old male with co-existing AS and SCD who underwent staged bilateral THA with good clinical and radiographic outcomes at 5 years follow-up. Co-existing AS and SCD can present unique intraoperative surgical challenges in patients undergoing THA as seen in our patient, and the establishment of perioperative management guidelines may help prevent complications.
Keywords: ankylosing spondylitis; sickle cell disease (SCD); total hip arthroplasty (THA); hip.
Citation: Shah VI, Pachore JA, Patil J, Rajani D, Shetty GM, et al. A rare coexistence of ankylosing spondylitis and SCD: Pitfalls and challenges during THA J Clin Images Med Case Rep. 2022; 3(3): 1729.
Introduction
Ankylosing Spondylitis (AS), a spondyloarthropathy that manifests as a chronic inflammatory disease of the axial skeleton, causes painful degenerative changes of the hip joints requiring Total Hip Arthroplasty (THA) [1]. However, AS may rarely co-exist with an inflammatory disease like rheumatoid arthritis, which may further worsen the patient’s hip disease and functional limitations [2].
Sickle Cell Disease (SCD) is an autosomal recessive Red Blood Cell (RBC) disorder causing the production of Abnormal Haemoglobin (Hb) and distortion of RBCs leading to vasoocclusion, hemolysis, and tissue ischemia [3]. Hence SCD can cause extensive bone infarcts and Osteonecrosis (ON) with hip arthritis in patients [3]. Although more common in the malaria-endemic regions of the world, the worldwide prevalence of sickle gene carriers ranges from 1%-35% [4,5].
Although AS and SCD are well known to cause severe hip arthritis [1,3], the co-existence of AS and SCD is extremely rare, with only one case reported in the literature [6]. Furthermore, the case of a patient with co-existing AS and SCD undergoing THA has never been reported. Hence, we report the case of a patient with an extremely rare co-existence of AS and SCD who underwent a staged bilateral THA for severe hip arthritis.
Case history
We obtained informed consent regarding the use of anonymized data concerning his case for research and publication from the patient for this study. A 39-year-old male patient, known case of AS, presented to our hospital with complaints of stiffness of both hips, difficulty in walking and carrying out daily routine activities for the past five years. On examination, the patient had a stooped posture with severe lower lumbar spine stiffness. In addition, both hips had a fixed flexion deformity (20° right and 10° left). Pelvis with both hips radiograph showed severe arthritis with concentric reduction of joint space and bilateral fusion of the sacroiliac joints (Figure 1).

After routine preoperative work-up, a THA was performed for the more severe right side. The right THA was performed using a standard posterior approach. After hip dislocation and neck osteotomy, significant difficulty was encountered during the attempt to enter the canal due to the presence of hard osteosclerotic medullary bone. After the initial attempt with a box chisel, the canal was entered by drilling from the piriformis fossa. A short guide wire was then inserted, and the canal was reamed using intramedullary reamers. After broaching and trial, a size 2, 12/14 taper uncemented femoral stem (Summit cementless stem, Depuy, Warsaw, IN) was implanted. Postoperative x-rays after the right THA revealed multiple diaphyseal sclerotic lesions in both femora, which suggested the coexistence of SCD in the patient. A subsequent Hb electrophoresis test confirmed SCD.
The left THA was planned 6 months after the right THA, and a preoperative CT scan of the left femur was done to visualise SCD changes in the bone (Figure 2).
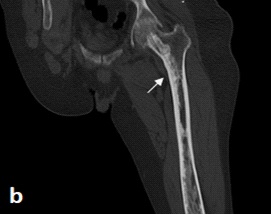
In view of the SCD, the patient underwent blood transfusion preoperatively to prevent intra- and postoperative complications related to excessive blood loss and anaemia. Based on the experience of the right THA and CT scan visualisation of intramedullary osteosclerotic changes, proper surgical instruments, incrementally sized reamers, and adequate implant sizes were kept ready for optimal canal preparation and femoral implantation. The femoral canal was prepared, and a size 4, 12/14 taper uncemented femoral stem (Summit cementless stem, Depuy, Warsaw, IN) was implanted. Postoperatively, the patient was given adequate fluid maintenance, oxygenation, and pain management to preventa Vaso occlusive crisis [3]. There were no intra- or postoperative complications seen in this patient.
Limb length discrepancy of 1.5 cm was noted on the right side at the 5 years follow up visit, and the postoperative radiograph taken revealed subsidence and femoral implant loosening on the right side with no abnormality on the left side (Figure 3).

Hence, femoral revision with the exchange of liner was carried out on the right side. A 2.5 cm cortical window was created intra-operatively in the shaft femur just distal to the tip of the stem and high-speed burr was used to remove the sclerotic bone, which aided in easier reaming and canal entry (Figure 4).

Revision surgery was done with Wagner SL Femur Revision Stem Size 14 × 265 (Zimmer Biomet), Delta ceramic femoral head size 28 mm/-3.5 mm (Zimmer) and Duraloc Marathon Acetabular Liner 10° (Depuy Synthes). There were no post-operative complications noted.
Discussion
Both AS and SCD can cause similar changes in the hip joint, including ON, severe arthritis, and ankylosis. Although the presence of AS in a patient undergoing THA can lead to difficulty in dislocation, increased risk of intraoperative fractures, and soft-tissue imbalance during surgery, the co-existence of SCD can further increase intraoperative challenges. Significant occlusion of the femoral canal may be encountered in SCD due to medullary narrowing and patchy sclerosis, which increases the difficulty in femoral canal preparation and femoral component implantation [7], as illustrated in this case report. In addition, canal occlusion also increases the risk of creating false passages, cortical perforation, and fracture during the preparation of the femoral canal [7], especially in the presence of co-existing AS. Hence, femoral canal dimensions should be assessed using preoperative CT scan, and proper surgical instruments and implants (uncemented and cemented) should be kept available during surgery.
Complications after THA such as postoperative wound infections, Deep Vein Thrombosis (DVT), and Pulmonary Embolism (PE) and have been reported to be more frequent in patients with SCD [8]. Hence appropriate measures to prevent infection such as adequate perioperative antibiotics coverage and thromboprophylaxis are essential in a patient with SCD undergoing THA. Furthermore, perioperative medical complications due to a vasoocclusive crisis and their risk factors such as decreased oxygen saturation, opioid-induced respiratory depression, hypovolemia, hypotension, and variations in body temperature must be kept in mind and prevented during THA [3].
Although AS is a common indication for THA, screening for SCD in these patients undergoing THA, especially in a population with a higher prevalence of SCD carrier gene, can help diagnose the coexistence of SCD with AS preoperatively. This case report highlights the importance of a thorough evaluation of preoperative x-rays to detect meta- and diaphyseal osteosclerotic lesions frequently seen in SCD which may go undiagnosed during the initial investigations. Given the technical difficulties which may be encountered intraoperatively and the increased risk of perioperative complications in such patients, a thorough preoperative evaluation is necessary and adequate intra- and postoperative preventive measures should be taken.
Conclusion
The rare coexistence of AS and SCD can present unique challenges in patients undergoing THA, and establishment of perioperative management guidelines for such cases will be helpful to minimise complications improve patient outcomes.
Declarations
Acknowledgements: None
Conflict of interests: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- Lin D, Charalambous A, Hanna SA. Bilateral total hip arthroplasty in ankylosing spondylitis: A systematic review. EFORT Open Rev. 2019; 4: 476-481.
- Zhang Y, Feng B, Dong J, Zhong Y, Wang L, Zhao L, et al. Rheumatoid arthritis coexisting with ankylosing spondylitis: A report of 22 cases with delayed diagnosis. Medicine (Baltimore). 2021; 100: e25051.
- Vanderhave KL, Perkins CA, Scannell B, Brighton BK. Orthopaedic Manifestations of Sickle Cell Disease. J Am Acad Orthop Surg. 2018; 26: 94–101.
- Colah R, Mukherjee M, Ghosh K. Sickle cell disease in India. Curr Opin Hematol. 2014; 21: 215-223.
- Kato GJ, Piel FB, Reid CD, et al. Sickle cell disease. Nat Rev Dis Primers. 2018; 4: 18010.
- Sívrí A, Ari C, Kutsal YG, Basgoze O, Ozker R. Evidence of coexisting spondyloarthropathy and sickle-cell disease. Scand J Rheumatol. 1992; 21: 310-311.
- Hug KT, Gupta AK, Wellman SS, Bolognesi MP, Attarian DE. Creation of a femoral cortical window to facilitate total hip arthroplasty in patients with sickle cell hemoglobinopathies. J Arthroplasty. 2013; 28: 323–325.
- Hernigou P, Housset V, Pariat J, Dubory A, Flouzat Lachaniette CH. 2020; Total hip arthroplasty for sickle cell osteonecrosis: Guidelines for perioperative management. EFORT Open Rev. 2020; 5: 641–651.