
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Twin-Twin Transfusion Syndrome (TTTS) in dichorionic-diamnionic twin pregnancy: A case report
Genxia Li1*; Shuhui Chu1; Linlin Zhang2; Shuo Feng1; Hezhou Li3; Li Dong3; Zhiwei Hao4; Yanxia Niu5; Haiyang Yu2; Kang Chen6
1 Obstetrics Department, The Third Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 450052.
2 Department of clinical Laboratory, The Third Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 450052
3 The Ultrasound Department, The Third Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 450052.
4 The Pathology Department, The Third Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 450052.
5 Obstetrics Department, Luan Chuan Maternal and Child Health Hospital, Luoyang, China, 471500.
6 Departments of Obstetrics and Gynecology, Oncology, Biochemistry, Microbiology and Immunology, Wayne State University, Detroit, MI 48201, USA.
*Corresponding Author: Genxia Li
Obstetrics Department, The Third Affiliated Hospital of Zhengzhou University, Zhengzhou, China,
450052.
Email: [email protected]
Received : Feb 11, 2022
Accepted : Mar 07, 2022
Published : Mar 14, 2022
Archived : www.jcimcr.org
Copyright : © Li G (2022).
Abstract
Twin-to-Twin Transfusion Syndrome (TTTS) is a serious complication of twin pregnancy, which develops in approximately 10 to 15 percent of monochorionic twin pregnancies while it is very rare in dichorionic pregnancies. At present, fetal laser surgery has become the preferred treatment for stage II to IV TTTS. It has been reported that fetal laser therapy after early diagnosis of TTTS can improve neonatal outcome. From May 2018 to December 2021, there are a total of 140 cases which underwent fetoscopic laser surgery in the Third Affiliated Hospital of Zhengzhou University. Among them, one case of twin-twin transfusion syndrome was dichorionic twins. The patient with dichorionic-diamnionic twin pregnancy was diagnosed with TTTS Stage II at 23 weeks and 4 days of Gestational Age (GA). After fetoscopic laser surgery and bipolar coagulation, the patient delivered vaginally two viable male infants at 31 weeks GA. Follow-up showed that the two infants survived.
Keywords: TTTS; dichorionic twins; fetoscopic; placenta.
Citation: Li G, Chu S, Zhang L, Feng S, Li H, et al. Twin-Twin Transfusion Syndrome (TTTS) in dichorionic-diamnionic twin pregnancy: A case report. J Clin Images Med Case Rep. 2022; 3(3): 1732.
Case report
A 35-year-old patient, gravida-5, para-2, was admitted at 23 4/7 weeks of gestation due to finding that her amniotic fluid was unevenly distributed for 1 day on October 10, 2018. The patient had a regular menstrual cycle. LMP April 28, 2018. Ultrasound during early pregnancy revealed a double pregnancy sac. Fetal ultrasound on admission showed: BPD: 62/56 mm; FL: 40/39 mm; AFV: 116.0/0 mm; S/D: 2.7/2.9. The two placentas were located in the anterior and posterior wall of the uterus respectively; A ribbon could be seen under ultrasound in the sac of the polyhydramnios fetus, and the edge of the two placentas were connected by the ribbon. On the recipient twin, his bladder was visualized and on the donor twin, the bladder was not visualized. Diagnosis: dichorionic-diamnionic twin pregnancy; TTTS of stage II; 23 weeks and 4 days GA; G5 P2.
Within 24 hours of admission, the patient underwent fetoscopic laser surgery after she gave written informed consent. During surgery, a fetoscope was placed into the amniotic cavity of the polyhydramnios sac. 20 ml of amniotic fluid was taken for Chromosomal Microarray Analysis (CMA), which revealed a 420 kb microdeletion on chromosomal band 16 p13.3, which was polymorphism of genes.
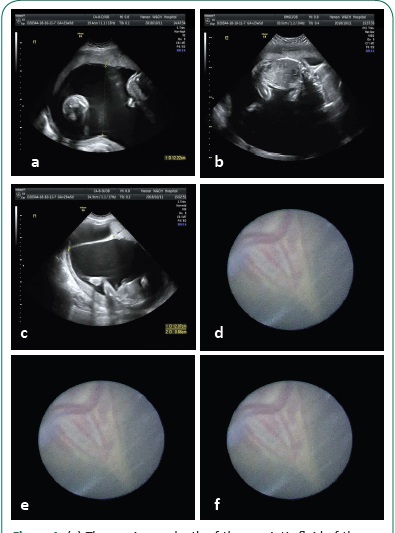
Under the fetoscope, the adhesive band was a 10 mm wide which was floating in the womb. At each end of the band, two thick blood vessels were noted, and in the middle, there were communicating vessels. Two placentas were well-defined. There was no other communicating branches found besides the adhesive band. The intraoperative ultrasound image was shown in Figure 1. During the operation, blood vessels on the end of the band from the placenta were coagulated by laser. To avoid the residual of the communicating vessels in the adhesion zone, the middle part of the adhesive band was solidified for 1-2 cm with visual bipolar electric coagulation forceps. Amniotic fluid was reduced by 1500 ml to ensure that the maximum depth of amniotic fluid became 80/0 mm. Gelatin sponge was placed into uterine wall of the puncture hole to prevent amniotic fluid leakage and bleeding. After observation for 30 minutes, the patient was returned to the ward without apparent abnormality. Cefazolin with intravenous drip was given to prevent infection for 24 hours after operation. Two hours after the operation, indomethacin suppository was used in rectal injection to prevent uterine contractions for 2 days. A transient amniotic fluid leak age occurred after operation. The patient was discharged on the postoperative day 3 when her amniotic fluid was normal and contraction and vaginal effluent were not found. Ultrasound was reviewed once a week. When ultrasound was normal for 3 weeks, routine perinatal care was performed.
Follow-up
The pregnant woman was readmitted at 31 weeks’ of gestation due to premature labor on December 1, 2018. She delivered vaginally two viable male infants on the same day. The recipient twin weighed 1460 grams and had Apgar scores of 8 and 9 at 1 and 5 minutes, respectively. The donor twin weighed 1580 grams and had Apgar scores of 8 and 9 at 1 and 5 minutes, respectively. They were transferred to the neonatal intensive care unit for treatment and discharged after 27 days. After delivery of the placenta, the area of the original adhesive band was noted. The placental perfusion showed complete blockage of communicating vessels, no residue (Figure 2), and the pathological examination of adhesion zone revealed no residual blood vessel. The suspected site of lesion of the adhesion band was selected through observation, then sliced and stained after paraffin blocks were made. Pathology of the placenta in this case showed highly suspected necrotic area (Figure 3). Molecular analysis using multiple polymorphic microsatellite centromeric markers [1-2] was performed on parental and the two infants’ blood samples. The results from 21 loci over the same number of chromosomes were consistent with monospermic fertilization of one ovum and eliminated the possibility of dizygotic twins.


Discussion
TTTS is a known and serious complication of monochorionic twin pregnancies [3]. There are also case reports suggesting that TTTS occurs in dichorionic-diamnionic twins [3-6]. In this case, an adhesion zone was generated between the placentas. We surmise that the placental adhesion zone was formed in the first trimester and the placental blood vessels grew into the zone in the second trimester, and anastomotic branches were formed thereafter. The separation of the zygote in the morula or late blastocyst is incomplete and there are still tissue or vascular Bridges between the two blastocysts.
The principle of TTTS in dichorionic-diamnionic twin pregnancy may be that the separation of zygote in morula or late blastocyst is incomplete, and there are still tissue or vascular bridge connections between the two blastocysts. In addition, it may be related to the failure of the mechanism that inhibits angiogenesis in the periplacental region.
We suggest that clinicians pay attention to the possibility of TTTS in a dichorionic twin pregnancy in case of the occurrence of adverse pregnancy outcomes due to the possibility of not making a timely diagnosis of TTTS. Discordance on the amount of amniotic fluid, differences in weight and bladder between the two fetuses is in favor of the diagnosis of TTTS [3]. Fetal laser surgery can also be considered for TTTS in dichorionic twin pregnancy in order to improve pregnancy outcomes. During the operation, appropriate blood flow blocking protocol can be selected according to the characteristics of connected tissues and blood vessels.
References
- Becker A, Busjahn A, Faulhaber DH, et al. Twin zygosity. Automated determination with microsatellites. [J]. The Journal of reproductive medicine. 1997; 42: 6-260.
- Erdmann J, Nothen MM, Stratmann M, Fimmers R, Franzek E, Propping P, et al. The use of microsatellites in zygosity diagnosis of twins. Acta Genet Med Gemellol (Roma). 1993; 42: 45–51.
- Cavazza Maria Carlota, Lai Ana-Catarina, Sousa Sílvia, et.al. Dichorionic pregnancy complicated by a twin-to-twin transfusion syndrome [J]. BMJ Publishing Group Ltd. 2019; 12: 1-3.
- Lanna M, Faiola S, Casati D, et.al. Twin-twin transfusion syndrome in dichorionic twin pregnancy rare but not impossible. Ultrasound in obstetrics & amp; gynecology: The official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2019; 54: 417-418.
- Quintero Ruben, Kontopoulos Eftichia V, Barness Enid, et.al. Twin-twin transfusion syndrome in a dichorionic-monozygotic twin pregnancy. The end of a paradigm [J]. Fetal & amp; Pediatric Pathology. 2010; 29: 81-88.
- Murata S, Takano M, Kagawa Y, Fujiwara M, Sumie M, Nakata M, et al. Twin-twin transfusion syndrome in a monozygotic pregnancy with obvious lambda sign in first-trimester ultrasound. Taiwan J Obstet Gynecol. 2016; 55: 904-906.