
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Unclassified testicular sex cord-stromal tumors in children
Armas Alvarez Azucena Lirio1; Osorio Manyari Angel Alois2; Moreno Pérez De la Cruz Santiago1; Abaigar Pedraza Irache1;Camacho Monge Juan José1; Pérez Holgado Victoria3; Pérez Cidoncha Pedro4; López de Alda González Andrés5
1 Urologist, Hospital de Don Benito-Villanueva de la Serena, Badajoz, Spain.
2 General Surgeon, Hospital de Don Benito-Villanueva de la Serena, Badajoz, Spain.
3 Pathologist, Hospital de Don Benito-Villanueva de la Serena, Badajoz, Spain.
4 Chief of the Pathology Department, Hospital de Don Benito-Villanueva de la Serena, Badajoz, Spain.
5 Chief of the Urology Department, Hospital de Don Benito-Villanueva de la Serena, Badajoz, Spain.
*Corresponding Author: Armas Alvarez Azucena
Lirio
Urologist at the Hospital de Don Benito-Villanueva
de la Serena, Badajoz, Spain.
Email: azli_1673@hotmail.com
Received : Feb 17, 2022
Accepted : Mar 09, 2022
Published : Mar 16, 2022
Archived : www.jcimcr.org
Copyright : © Armas Alvarez AL (2022).
Abstract
We report a case of 12-year-old boy diagnosed with an unclassified sex cord stromal testicular tumor after a mild testicular trauma and the unclear ultrasound finding of a testicular mass. Physical examination was significant for a mass in the right testis. Scrotal magnetic resonance revealed an 8 millimeters nodular lesion suggestive of a Leydig cell tumor. Tumor markers were negative. The patient underwent a right radical orchiectomy plus implantation of a testicular prosthesis. Tumor cells expressed inhibin, WT 1, CD 56, CD99, vimentin and actin. Pathological diagnosis was unclassified sex cord stromal tumor confined to the testis. Metastatic workup by CT was negative.
Unclassified sex cord-stromal tumors are infrequent and show an indeterminate differentiation of tumor cells that cannot be characterized with light microscopy towards Leydig, Sertoli, granulosa or theca cells. Immunohistochemistry helps in the differential diagnosis.Due to the risk of malignancy, local recurrence and uncertain biological behavior, radical orchiectomy is recommended, and a metastatic workup should be performed.
Keywords: children; orchiectomy; sex cord-stromal tumor; scrotal ultrasound; testicular tumor.
Citation: Armas Alvarez AL, Osorio Manyari AA, Moreno Pérez De la Cruz S, Abaigar Pedraza I, Camacho Monge JJ, et al. Unclassified testicular sex cord-stromal tumors in children. J Clin Images Med Case Rep. 2022; 3(3): 1740.
Introduction
Testicular tumors are infrequent in boys and within these, unclassified sex cord-stromal tumors constitute 5% [1].
Due to its low frequency and limited description of this type of tumor in the literature, its treatment, prognosis, and followup are not completely defined [2].
We report a case of 12-year-old boy diagnosed with an unclassified sex cord-stromal testicular tumor after a mild testicular trauma and the ultrasound finding of a testicular mass.
Clinical case
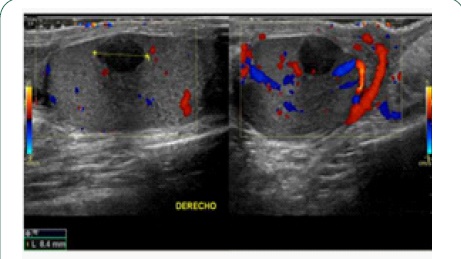
A 12-year-old boy with no history of interest presented pain in the right hemiscrotum for 4 days after mild testicular trauma. Physical examination was significant for a 1 cm firm mass in the right testis. Normal left testis. Scrotal ultrasound revealed an intensely hypoechoic nodular lesion measuring 8 X 6 mm.
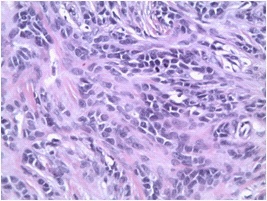
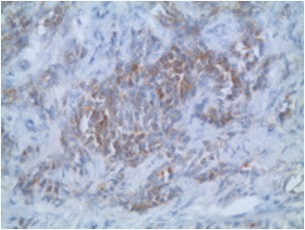
In the middle of the right testicular parenchyma, suggestive of an inclusion cyst versus testicular tumor (Figure 1). Scrotal MRI revealed an 8 millimeters nodular lesion in the right testis isointense on T1 and hypointense on T2, suggestive of a Leydig cell tumor (Figure 2). Tumor markers were negative. The patient underwent a right radical orchiectomy plus implantation of a testicular prosthesis. Pathological diagnosis was unclassified sex cord stromal tumor of 8 mm confined to the testis without margin involvement or lymphovascular invasion (Figure 3). Immunohistochemically, tumor cells expressed inhibin, WT 1, CD 56, CD99, vimentin and actin (Figure 4). Metastatic workup by CT was negative. The follow-up at 12 weeks, he was well, tumor markers were normal, and the ultrasound showed a normal left testis.

Discussion
Testicular tumors constitute 1-2% of solid neoplasms in children [3]. The most common symptoms are a painless scrotal swelling or a palpable mass [4]. There may be testicular pain that is associated with testicular hemorrhage or necrosis. A history of trauma, hernia or hydrocele occurs in less than 10% of cases. Our patient had a mild testicular trauma after which he presented testicular pain, so an ultrasound was performed which showed a testicular mass.
The diagnosis of a testicular mass relied on the determination of serum markers: Beta hCG, alpha fetoprotein and lactate dehydrogenase, and imaging studies such as ultrasound and MRI.
Ultrasonography has a sensitivity of 100% for detecting testicular neoplasms and a specificity of less than 15% except in testicular cysts [5].
Scrotal MRI is used to characterization of the tumors when US findings are indeterminate and help in differentiating between germ cell tumors and non-germ cell tumors.
In our case, the ultrasound was inconclusive, so a testicular MRI was performed which detected the testicular tumor.
Staging is done with MRI and chest radiography or CT.
MRI is preferred due to concerns for radiation exposure with CT imaging [6]. If CT is used, it is recommended to reduce the radiation dose.
In children, 65-75% of testicular tumors are germ cell tumors and 5-15% are of stromal origin. Sex cord-stromal tumors can be Leydig cell, Sertoli cell, granulosa and theca cell, mixed tumors, and unclassified tumors [7].
Stromal tumors are hormonally active causing precocious puberty and gynecomastia in 10% of cases and they are associated with syndromes such as Peutz-Jeghers, Carney Complex, among others in 30% [2].
Unclassified sex cord-stromal tumors account for 5% of testicular tumors in prepubertal boys [1]. These tumors show an indeterminate differentiation of tumor cells that cannot be characterized with light microscopy towards Leydig, Sertoli, granulosa or theca cells [8,9].
Immunohistochemistry helps in the differential diagnosis. The reactivity for S100, smooth muscle actin, inhibin and vimentin has been shown to be reliable with the diagnosis of this type of testicular tumor [9].
In our case, the tumor cells expressed inhibin, vimentin, actin and S100.
Unclassified stromal tumors are malignant in 10% of cases [1,10]. The histological characteristics associated with malignancy are large size (greater than 5 cm), infiltrative borders, high mitotic activity (more than 3 mitoses/10 high power fields), vascular or lymphatic invasion, significant nuclear atypia, and necrosis [4]. The biological behavior and prognosis of unclassifiable stromal tumors are difficult to predict [7,10,11].
Due to the risk of malignancy, local recurrence and uncertain biological behavior, radical orchiectomy is recommended as treatment [2,7]. And since these tumors can exhibit metastatic activity, a metastatic workup should be performed.
Testis sparing surgery has been described with a disease-free status, although follow-up was short (4 months to 1 year) [12]. Its advantage is the lack of hormonal and reproductive dysfunction that occurs in unilateral radical orchiectomy.
A longer follow-up time is required to confirm the absence of recurrence to be able to consider it as a treatment in this type of tumor.
Follow-up should be close and long term since late recurrences have been described 15 years after diagnosis and to document male sexual development, psychological well-being, quality of life and reproductive health [1,13]. Laboratory tests with tumor markers and imaging studies such as CT, MRI and ultrasound are used.
There is no consensus on adjuvant treatment with chemotherapy and radiotherapy and retroperitoneal lymphadenectomy
Conclusions
Unclassified sex cord stromal testicular tumors are rare. They are at risk of malignancy, so radical orchiectomy and metastatic workup are recommended. Follow-up should be close and longterm using laboratory tests and imaging studies, preferably ultrasound and MRI in children.
Declarations
Confidentiality of data: The authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent: the authors declare that no patient data appear in this paper.
Conflict of interests: All authors declare they have no conflict of interest.
References
- Brekelbaum CE, Abreo F, Fowler M, Kubricht WS, Eastham JA. Undifferentiated sex cord/stromal testis tumor. Urology. 2000; 55: 436xvii-xviii.
- Hofmann M, Schlegel PG, Hippert F, Schmidt P, Von-Schweinitz D, Leuschner I, et al. Testicular sex cord stromal tumors: Analysis of patients from the MAKEI study. Pediatr Blood Cancer. 2013; 60: 1651-1655.
- Maizlin II, Dellinger M, Gow KW, Goldin AB, Goldfarab M, Nuchtern JG, et al. Testicular tumors in prepubescents patients. J Pediatr Surg. 2018; 53: 1748-1752.
- Thomas JC, Ross JH, Kay R. Stromal testis tumors in children: A report from the prepubertal testis tumor registry. J Urol. 2001; 166: 2338-2340.
- Stein R, Quaedackers J, Bhat NR, Dogan HS, Nijman RJM, Rawashdeh YF, et al. EAU_ESPU pediatric urology guidelines on testicular tumors in prepubertal boys. J pediatr Urol. 2021; 17: 529-533.
- Tsili AC, Sofikitis N, Stiliara E, Argyropoulou MI. MRI of testicular malignancies. Abdom Radiol. 2019; 44: 1070-1082.
- Goswitz JJ, Pettinato G, Manivel JC. Testicular sex cord-stromal tumors in children: clinicopathologic study of sixteen children with review of the literature. Pediatr Pathol Lab Medicine 1996; 16: 451-470.
- Idrees MT, Ulbright TM, Oliva E, Young RH, Montironi R, Egevad L, et al. The world health organization 2016 Classifi-cation of testicular non-germ cell tumours: A review and update from the international society of urological pathology testis consultation panel. Histopathology. 2017; 70: 513-521.
- Sajadi KP, Dalton RR, Brown JA. Sex cord gonadal stroma tumor of the rete testis. Adv Urol. 2009; 2009: 624173.
- Tarjan M, Sarkissov G, Tot T. Unclassified sex cord gonadal stromal testis tumor with predominance of spin-dle cells. APMIS. 2006; 114: 465-469.
- Yang DT, Lowichik A, Chen J, Snow BW, Ulbright TM, Chen Z. Cytogenetics of a pediatric unclassified sex cord-stromal tumor of the testis: a case report. Cancer Genet Cytogenet. 2005; 156: 80-82.
- Woo LL, Ross JH. The role of testis sparing surgery in children and adolescents with testicular tumors. Urol Oncol. 2016; 34: 76-83.
- Liu SYW, Ng CF, Lai FMM, Cheng CW. Undifferentiated sex cordstromal tumors in a young adult. Int Urol Nephrol. 2007; 39: 561-564.