
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Thoracoscopic removal of a posterior mediastinal parathyroid adenoma
Hazem Zribi1; Mariem Hadj Dahmane1*; Imen Bouassida1; Mahdi Abdennadher1; Dorra Ben Sellem2; Amira Dridi3; Faouzi E1Mazni4; Adel Marghli1
1 Thoracic Surgery Department, Abderrahmen Mami University Hospital, Ariana, Tunisia
2 Nuclear Medicine Department, Salah AZAIEZ Institute, Tunis, Tunisia.
3 Anesthesiology and Reanimation Department, Abderrahmen Mami University Hospital, Ariana, Tunisia.
4 Department of Anatomical Pathology, Abderrahmen Mami University Hospital, Ariana, Tunisia.
*Corresponding Author: Mariem Hadj Dahmane
Thoracic Surgery Department, Abderrahmen Mami
University Hospital, Ariana, Tunisia.
Email: mariamhajd@gmail.com
Received : Feb 18, 2022
Accepted : Mar 09, 2022
Published : Mar 16, 2022
Archived : www.jcimcr.org
Copyright : © HadjDahmane M (2022).
Abstract
Ectopic Parathyroid Adenomas (EPA) can occur in many anatomical locations and the most frequent one was the mediastinum region. Traditionally, the adenoma resection has been performed through conventional thoracotomy or sternotomy. Recently, a few cases of thoracoscopic excision of mediastinal adenoma were reported. We report here the case of a successful exclusive thoracoscopic removal of a mediastinal parathyroid adenoma. A 58-year-old female patient presented with bilateral renal stones and fatigue. Biology results showed elevated serum calcium and parathyroid hormone levels. The diagnosis of primary hyperparathyroidism caused by solitary EPA in lateralesophageal region was confirmed by imaging tools. The patient underwent successful thoracoscopic resection. He was discharged on the 2rd postoperative day.
Keywords: primary hyperparathyroidism; parathyroid adenoma; mediastinum; thoracoscopic excision.
Abbreviations: EPA: Ectopic Parathyroid Adenomas; PHPT: Primary Hyperparathyroidism; PTH: Parathyroid Hormone; CT: Thoracic Computed Tomography; SPECT/CT: Single-Photon Emission Computed Tomography with Computed Tomography
Citation: Zribi H, HadjDahmane M, Bouassida I, Abdennadher M, BenSellem D, et al. Thoracoscopic removal of a posterior mediastinal parathyroid adenoma. J Clin Images Med Case Rep. 2022; 3(3): 1741.
Introduction
Ectopic parathyroid adenomas are the cause of Primary Hyperparathyroidism (PHPT) approximately in 20% of cases [1]. This pathology is the result of aberrant migration of the parathyroid gland during development [2]. Mediastinum is the most common ectopic localization. The first report of a mediastinal EPA was in 1932 by Churchill [2]. The approach has traditionally been performed by conventional thoracotomy or sternotomy. Actually, the approach has vastly changed. Several published reports and case series have described successful thoracoscopic excision using video-assisted thoracoscopic surgery [3].
We present our case of a successful thoracoscopic removal of a rare upperposterior mediastinal parathyroid adenoma, and suggest that this approach is a viable alternative in patients with this disease.
Case report
A 58-year-old female patient presented with fatigue, somnolence, and anorexia. The patient was operated for bilateral renal stones. The biology results showed elevated serum calcium 4.6 mmol/L (N 2–2.6 mmol/L) and Parathyroid Hormone (PTH) 410 pg/ml (15-65 pg/ml). The other laboratory tests were within the normal range and the patient was diagnosed with PHPT.
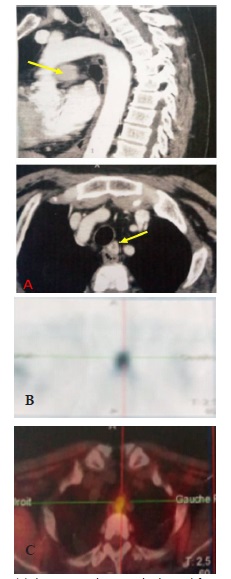
A thoracic Computed Tomography (CT) revealed a well-defined oval-shaped soft tissue in the posterior mediastinum at the level of the third thoracic vertebra in the left upper posterior mediastinum adjacent to the oesophagus (Figure 1A). A dual-phase dual-tracer parathyroid scintigraphy with MethoxyIsoButyl Isonitrile labelled with Technetium-99m (99m Tc-MIBI) was performed. Planar images (Figure1B) and single-photon emission computed tomography with computed tomography (SPECT/CT) ones (Figure 1C) objectified an obvious focal radiotracer accumulation in the posterior mediastinum. These findings were consistent with a mediastinal EPA.
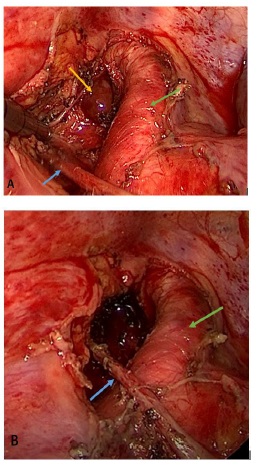
The patient underwent left thoracoscopic exploration, she was intubated with a double lumen endotracheal tube and placed in the right lateral decubitus position. The procedures were performed through one 12-mm camera port introduced in the fourth intercostal space in the mid-axillary line and two 5-mm operating ports. Thoracoscopy revealed a mass approximately 12 mm in length in the posterior mediastinum, which was subsequently resected. Finding the adenoma deep in the posterior mediastinum was not easy. Careful dissection of the mediastinal tissue adjacent to the left subclavian artery was performed, taking care not to damage the right vagal nerve (Figure 2A). Thoracoscopy revealed a brown tumor measuring 12 X 10 mm that looked distinct from lymph nodes. The adenoma was observed under the left subclavian artery and was then dissected using the diathermy hook and removed intact, without fracture of its capsule, using a sample collection bag. At the end of the operation, a chest tube was inserted after the lung was re-inflated. The surgical specimen consisted of brown soft tissue and histology confirmed an intact parathyroid adenoma.
The chest tube was removed 1 day postoperatively and the patient was discharged on the second day. The postoperative course was uneventful. Serum level of calcium and PTH were normalized on 1 day postoperatively. At a follow-up, two weeks after surgery, the patient had normal serum calcium level and no complications.
Discussion
Primary hyperparathyroidism is a rare disease, that mainly caused by a solitary parathyroid adenoma [4,5]. This adenoma was located in the thyroid or in ectopic locations which are caused by aberrant embryological migration of the parathyroid gland. The most frequent ectopic localization is mediastinal [4].
The most common symptoms of EPA are the symptoms of chronic hypercalcemia. Symptoms range from fatigue, vomiting, constipation, calculus, polyuria, memory loss, poor concentration. The major long-term complications are acute pancreatitis, kidney damage and osteoporosis [1]. The severity of symptoms correlates with the hyper functioning adenoma [1].
Preoperative localization of the adenoma is important for successful mini-invasive resection. Parathyroid scintigraphy has historically been the most commonly used imaging modality to localize EPA [6,7]. Recently, the use of hybrid machines SPECT/ CT has improved the performance of planar imaging [4,8]. In fact, SPECT/CT provides better anatomic detail by identifying the three-dimensional localization of the parathyroid gland, especially in the ectopic position. Nevertheless, it delivers an additional radiation dose. In our case, the location of abnormal parathyroid glands was determined by CT and 99 m Tc-MIBI parathyroid SPECT/CT.
The main indications for surgery resection of EPA are glandular hyperfunction, complications from hypercalcemia, and young age of the patient [1].
Conventional approaches for mediastinal EPA are sternotomy, or thoracotomy. These approaches have been largely associated with significant complications as well as phrenic and recurrent laryngeal nerve injuries, innominate vein laceration, mediastinitis, and death [2]. Many mini-invasive approaches can be found in the literature, including subxiphoid laparoscopy, mediastinoscopy, and transcervical anterior mediastinal exploration using sternal retractor. However, these approaches are not the best to follow in order to obtain a good exposure of all the mediastinum regions [3]. Since the first account of thoracoscopic resection of a mediastinal EPA by Prinz et al in 1994, many case series have been reported success in using the same approach [3]. Thoracoscopic approach is now more widely used to remove mediastinal EPA located deep in the mediastinum, with minimally complications [1,2]. A review of the current literature confirms that exclusive thoracoscopy can provide excellent access to all mediastinal locations of adenoma and associated with lower rates of postoperative complications [3]. Thoracoscopic approach reduce also days of stay, postoperative pain and improved Cosmesis.
Conclusion
In conclusion, we believe that, in the hands of experienced surgeons and specialized centre of thoracic surgery, thoracoscopic can be a safe and successful approach for the management of mediastinal EPA.
Declarations
Conflicts of interest: The authors declare that there is no conflict of interests regarding the publication of this paper.
Acknowledgements: Not applicable.
Funding: There was no financial support
Ethics approval and consent to participate: The study was approved by the Ethical Committee of Abderrahmen Mami Hospital.
Consent for publication: The patient granted written informed consent for publication of this manuscript and the accompanyingimages.
References
- El Oueriachi F, Arsalane A, Kabiri EH. Adenoma paratiroideo ectópico poco frecuente. Arch Bronconeumol.2015; 51: 301-309.
- Hu J, Ngiam KY, Parameswaran R. Mediastinal parathyroid adenomas and their surgical implications. Ann R Coll Surg Engl. 2015; 97: 259-261.
- Chae AW, Perricone A, Brumund KT, Bouvet M. Outpatient Video-Assisted Thoracoscopic Surgery (VATS) for ectopic mediastinal parathyroid adenoma: a case report and review of the literature. J Laparoendosc Adv Surg Tech A. 2008; 18: 383-390.
- Zeng Z, Liao H, Luo F, Lin F. Mediastinal ectopic parathyroid adenoma. QJM. 2019; 112: 127-128.
- Taghavi Kojidi H, Vagharimehr N, Mohseni S, Pajouhi M, Mohajeri-Tehrani MR, et al. Unusual Ectopic Parathyroid Adenoma: A Case Report. Acta medica Iranica. 2016; 54: 547-550.
- Parikh AM, Suliburk JW, Morón FE. Imaging localization and surgical approach in the management of ectopic parathyroid adenomas. Endocr pract. 2018; 24: 589-598.
- Morón FE, Parikh AM, Suliburk JW. Imaging Ectopic Parathyroid Adenomas. A Literature Review. Rev. Colomb. Radiol. 2019; 30: 5069-5080.
- Beheshti M, Hehenwarter L, Paymani Z, Rendl G, Imamovic L, Rettenbacher R, et al. (18) FFluorocholine PET/CT in the assessment of primary hyperparathyroidism compared with (99 m) TcMIBI or (99 m)Tc-tetrofosmin SPECT/CT: a prospective dualcentre study in 100 patients. Eur J Nucl Med Mol Imaging 2018.