
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Caseous calcification of the mitral annulus presenting with symptomatic complete heart block
Mohammad Hossein Nikoo1; Sina Danesh2*; Firoozeh Abtahi3
1 Associated Professor of Cardiology, Shiraz University of Medical Science, Non-Communicable Diseases Research Center, Iran.
2 Health Policy Research Center, Institute of Health, Shiraz University of Medical Sciences, Shiraz, Iran.
3 Cardiology Department, Cardiovascular Research Center Shiraz University of Medical Sciences, Iran.
*Corresponding Author: Sina Danesh
Health Policy Research Center, Institute of Health,
Shiraz University of Medical Sciences, Shiraz, Iran.
Email: sina.danesh0670@gmail.com
Received : Dec 24, 2021
Accepted : Mar 10, 2022
Published : Mar 17, 2022
Archived : www.jcimcr.org
Copyright : © Danesh S (2022).
Citation: Nikoo MH, Danesh S, Abtahi F. Caseous calcification of the mitral annulus presenting with symptomatic complete heart block. J Clin Images Med Case Rep. 2022; 3(3): 1743.
Introduction
Mitral Annular Calcification (MAC) could even be a chronic, degenerative process of the fibrous support structure of the mitral valve [1,2]. MAC is usually visualized on echocardiography as an echo-dense shelf-like structure with an irregular, lumpy appearance involving the mitral valve annulus, with associated acoustic shadowing. within the Cardiovascular Health Study [3], MAC was quantified as mild (focal, limited increase in echodensity of the mitral annulus), moderate (marked echodensity involving one third to a minimum of 1 half the ring circumference), or severe (marked echodensity involving quite half the ring, or with intrusion into the left ventricular [LV] inflow tract).
MAC could also be a fibrous, degenerative calcification of the mitral valve support ring [4,5]. It had been first described in 1908 by Bonninger [6] in its association with complete heart block. Since then, it has been associated with endocarditis [7], coronary artery disease [8-12], and congestive heart failure [13- 15] in several studies, which mostly are small and retrospective in design. during a prior prospective investigation from the Framingham Heart Study, MAC was independently associated with stroke [16].
Diagnostic considerations
Three methods are available for the detection of MAC. The chest x-ray examination may be a rather insensitive method. Image intensification fluoroscopy has been shown to possess high sensitivity in diagnosing cardiac calcification. Echocardiography may be a useful and reliable noninvasive tool in detecting MAC [2,17].
Roentgenographic sensitivity and specificity are often improved by fluoroscopy. Image intensification fluoroscopy has been shown to detect about very small amounts of calcium, in contrast to autopsy studies during which special roentgenographic techniques are wont to evaluate the guts postmortem. Since calcification within the mitral anulus frequently progresses to massive proportions, it seems unlikely that image intensification fluoroscopy wouldn’t detect patients with this condition. The likelihood that occult “precalcific” mitral annular calcium accounts for the fluoroscopically negative cases remains unexplored [18,19].
Anatomy and pathology
The Mitral Valve (MV) annulus features a complicated threedimensional shape analogous to a saddle with the relative nadirs of the annulus located medially and laterally. At rock bottom of the LV, the annulus could also be a C-shaped segment of the fibrous skeleton. The MV leaflets are suspended from the mitral annulus, which provides structural support to the valve apparatus along the medial, posterior, and lateral aspects of the valve. Anteriorly, the midsection of the anterior mitral leaflet is in fibrous continuity with the posterior aortic root via the intervalvular fibrosa, without intervening annular tissue. In systole, normal mitral annular contraction is along the anteroposterior plane, resulting in folding along the mediolateral plane with a reduction in annular cross-sectional area, and facilitation of leaflet coaptation [20,21]. Three-dimensional echocardiography studies in patients with MAC have shown a relative loss of annular systolic motion, resulting in a much bigger, flatter annulus in systole [22].
Prevalence of MAC
The prevalence of MAC varies from 5% to 42% relying on the imaging modality used, the age and sex of the population studied and thus the frequency of associated risk factors. Within the Jackson Cohort of the Atherosclerotic Risk In Communities study (ARIC), a population-based echocardiographic study with mean age of 59 ± 6 years including African American participants, overall prevalence of MAC was 5.6% in men and 4.6% in women [23]. Within the Multi-Ethnic Study of Atherosclerosis (MESA), a cohort free of disorder at baseline with mean age 62 ± 10 years imaged by CT, the overall prevalence was 9%, with the absolute best prevalence in whites (12%), followed by Hispanics (10%), African Americans (7%) and Chinese Americans (5%) [24]. Within the Framingham Study, the echocardiographic M-mode prevalence of MAC with mean age 70 ± 5 years was 10.3% in men and 15.8% in women [16]. A high MAC prevalence of 42% was found within the Cardiovascular Health Study, which is that the oldest cohort examined by 2D echocardiography with a mean age of 76 ± 5 years. Similarly, MAC prevalence varies greatly when examined in referral-based, autopsy or surgical series [16].
Sex-related differences
Contrary to the atherosclerosis paradigm, several studies have found that female sex is claimed to an increased risk of developing MAC [24-26]. On the thought of his systematic pathological evaluation of 200 patients with MAC, Roberts [27] concluded that larger deposits are more frequent in women, although MAC of any degree appears to occur with similar frequency in men and ladies. It has been suggested that MAC in elderly women are often attributed to ectopic calcium deposits Contrary to the atherosclerosis paradigm, several studies have found that female sex is claimed to an increased risk of developing MAC [24-26]. On the thought of his systematic pathological evaluation of 200 patients with MAC, Roberts [27] concluded that larger deposits are more frequent in women, although MAC of any degree appears to occur with similar frequency in men and ladies. It has been suggested that MAC in elderly women are often attributed to ectopic calcium deposits
The large discrepancy in MAC prevalence between MESA and CHS relates mostly to differences in age but can also owe to the numerous imaging modalities used. Echocardiography could also be a smaller amount sensitive and doesn’t distinguish between fibrosis and calcification, while CT readily identifies calcium and enables quantification by the Agatston method [3]. An instantaneous comparison between methods is lacking.
The large discrepancy in MAC prevalence between MESA and CHS relates mostly to differences in age but can also owe to the numerous imaging modalities used. Echocardiography could also be a smaller amount sensitive and doesn’t distinguish between fibrosis and calcification, while CT readily identifies calcium and enables quantification by the Agatston method [3]. An instantaneous comparison between methods is lacking.
Risk factors
Factors that increase stress on the bicuspid valve and its surrounding structures increase the prospect of bicuspid valve calcification. the next conditions are related to development of mitral annular calcification [26]. Female sex, Older Age, Hypertension, mitral valve Prolapse, cardiomyopathy, Chronic kidney disease, Atherosclerosis, conditions predisposing to LV hypertrophy including hypertension and stenosis [30,31].
Complications
Several studies have verified the association of mitral annular calcification and thus the event of cardiac and other events. There’s increased risk of heart attacks, stroke and death from cardiovascular causes. There’s also an increased risk of development of fibrillation with RVR, an irregular cardiac rhythm. The danger is probably explained by the actual undeniable fact that patients with mitral annular calcification have risk factors for disorder. The presence of the calcium itself is unlikely dangerous [8,32].
The presence of mitral annular calcium makes it harder for surgeons to repair the bicuspid valve, as surgery is technically tougher. The calcium within the annulus can make the flexible valve more rigid and predispose to a leaky valve, however that’s usually not significant. Mitral annular calcification isn’t related to obstruction to blood flow and thus typically won’t have symptoms [33,34].
Treatment of mitral annular calcification
Mitral annular calcification is typically of no clinical significance and no specific treatment like Mitra Clip is required. Those with mitral annular calcification are at increased risk of cardiac events, although this is often still relatively small, likely thanks to the presence of traditional cardiac risk factors. Therefore it’s reasonable to advise those with mitral annular calcification to concentrate to sign, cholesterol, lifestyle, smoking, diabetes and other common risk factors. This might serve to scale back overall cardiac risk [35-37].
Case report
A 77-year-old man was referred to our centre with cc of mild vertigo, related to exertion and bradycardia that found accidentally in routine evaluation. He had a background medical record of chronic cough (describe as allergic) controlled glaucoma. He had features a history of Pos Cardiac Disease in his family (IHD (old age) & HTN in mother) and features a surgical history of appendectomy 15 years ago.
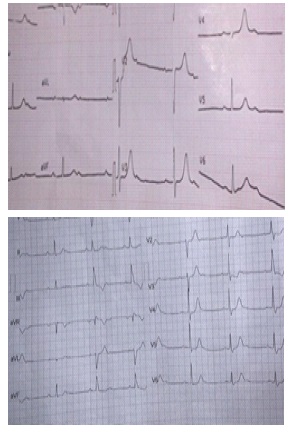
The electrocardiogram showed complete Adams-Stokes syndrome with a ventricular rate of 42 beats per minute and a narrow QRS escape rhythm of 146 ms (Figure 1A). Serum troponin wasn’t elevated (Figure 1).

His symptoms were as follows:
Sign was 145/85, pulse and rate of respiration were 40 and 18, respectively, and thus the temperature and amount of saturated oxygen were 36.5°C and 98% without O2 supplement, respectively. Left and Right ventricular size and performance, Left and Right Atrial size was normal. The left Ventricular Ejection Fraction was 55% without RWMA. Aorta was normal size without sign of dissection or flap. No visible cloth, no pericardial effusion and no other valular pathology were observed.
Fluoroscopy showed large deposits of calcium within the planet of the mitral annulus in patient. The mitral annulus is that the “c” shaped tissue at the left atrio-ventricular junction to which the mitral leaflets were attached. It was absent anteriorly where the mid portion of the anterior mitral leaflet was in fibrous continuity with the guts valve leaflets. Progressive deposition of calcium beneath and along the mitral annulus leads to mitral annular calcification. The calcification features a characteristic “c” shaped annulus sparing rock bottom of the anterior mitral annulus and was more commonly found in patients older than 70 years and in women. Mitral annular calcification was typically diagnosed on fluoroscopy as in our case.
Discussion
Mitral Annulus Calcification (MAC) could also be a chronic, degenerative process within the fibrous base of the mitral valve [30]. Initially thought to be an age-related degenerative process, there’s accumulating evidence that other mechanisms, like atherosclerosis and abnormal calcium-phosphorus metabolism, also contribute Reported prevalence of MAC is between 8% and 15%, but it significantly increases with age and in patients with multiple cardiovascular risk factors or Chronic Renal Disorder (CKD) MAC more commonly affects the posterior annulus than the anterior annulus [38].
The presence of a calcified mitral annulus is asymptomatic, which precludes true evaluation of the prevalence of MAC within the overall population. Despite its frequency, the clinical relevance of MAC is grossly under appreciated. In large historical autopsy studies, MAC was found in approximately 10% of patients.
CT scans or echocardiography assessments of MAC without defining its severity revealed calcification in 8% to fifteen of patients without known CVD. The prevalence of MAC was 42% in elderly patients with known CVD. A chest x-ray might reveal calcific demarcation of the mitral annulus & is typically seen as a C-, J-, U- or O- shape, with the open part lying at the location of the aortic outflow tract. Lateral projection usually better demonstrates mitral calcification because the overlying spine and main left lower lobe arteries within the posteroanterior view may mask its visualization [39,40].
Fluoroscopy during coronary angiography can also show mitral calcification, but isn’t an accurate modality. Generally has little or no effect on LV inflow or bicuspid valve function because, unlike in rheumatic mitral involvement, there is usual sparing of the leaflet commissures in these patients. Movahed et al. examined 24,380 echocardiograms and located MAC to be present in 11.7% of patients with MR versus 4.3% without MR [39,41].
A possible mechanism for this association is that calcium infiltration of rock bottom of the posterior leaflet reduces leaflet mobility, increases traction on the chordae, and elevates the leaflets. This facilitates chordal elongation or rupture, causing secondary MR. An alternate mechanism is failure of the calcified annulus to contract at the highest of diastole. Mitral valve stenosis because of annular calcification is reported to be quite rare. Nonetheless, it had been demonstrated that severe MAC could produce an enormous resting gradient across the mitral valve, thus causing bicuspid valve stenosis [42].
Patients with MAC have higher prevalence of Adams-Stokes syndrome, bundle branch block, and intraventricular conduction delay.
In our case the CV-SCAN report was Coronary artery calcium score was 23 in mid part of LAD in agatston unit. Massive crescent shape calcification was seen in mitral valve annulus involved inferior and lateral aspects of the ring of mitral valve extended to the posterior aspect of the aortic valve annulus. A central core of low attenuation area was seen in the calcified mass indicatied central necrosis or liquefaction. Extension of calcification was also evident in basal segment of the inferior wall of the left ventricle.
Conclusion
Our case demonstrates an old patient who had presented with Caseous calcification of the mitral annulus presenting with symptomatic complete heart block. Although echocardiography is usually sufficient to diagnose the condition, further evaluation with a Fluoroscopy was needed in this case to arrive at the diagnosis, suggesting the utility for Fluoroscopy in diagnostically complex cases.
References
- Korn D, De Sanctis RW, Sell S. Massive calcification of the mitral annulus: A clinicopathological study of fourteen cases. New England Journal of Medicine. 1962; 267: 900-909.
- Nestico PF, et al. Mitral annular calcification: Clinical, pathophysiology, and echocardiographic review. American heart journal. 1984; 107: 989-996.
- Barasch E, et al. Clinical significance of calcification of the fibrous skeleton of the heart and aortosclerosis in community dwelling elderly. The Cardiovascular Health Study (CHS). American heart journal. 2006; 151: 39-47.
- D’Cruz I, et al. Submitral calcification or sclerosis in elderly patients: M mode and two dimensional echocardiography in “mitral anulus calcification”. The American journal of cardiology. 1979; 44: 31-38.
- Hirschfeld DS, Emilson BB. Echocardiogram in calcified mitral anulus. The American journal of cardiology. 1975; 36: 354-356.
- Bonninger M. Bluttransfusion bei pernizioser anamie: (b) Zwei Falle von Herzblock. Dtsch Med Wochenschr. 1908; 34: 2292.
- Burnside JW, Desanctis RW. Bacterial endocarditis on calcification of the mitral anulus fibrosus. Annals of internal medicine. 1972; 76: 615-618.
- Jeon DS, et al. Association of mitral annulus calcification, aortic valve sclerosis and aortic root calcification with abnormal myocardial perfusion single photon emission tomography in subjects age≤ 65 years old. Journal of the American College of Cardiology. 2001; 38: 1988-1993.
- Tenenbaum A, et al. Advanced mitral annular calcification is associated with severe coronary calcification on fast dual spiral computed tomography. Investigative Radiology. 2000; 35: 193- 198.
- Adler Y, et al. Mitral annular calcium detected by transthoracic echocardiography is a marker for high prevalence and severity of coronary artery disease in patients undergoing coronary angiography. The American journal of cardiology. 1998; 82: 1183- 1186.
- Adler Y, et al. Mitral annular calcium detected by transthoracic echocardiography is a marker for high prevalence and severity of coronary artery disease in patients undergoing coronary angiography. The American journal of cardiology. 1998; 82: 1183- 1186.
- Gardin JM, et al. M-mode echocardiographic predictors of six-to seven-year incidence of coronary heart disease, stroke, congestive heart failure, and mortality in an elderly cohort (the Cardiovascular Health Study). The American journal of cardiology. 2001; 87: 1051-1057.
- D’Cruz IA, et al. Clinical manifestations of mitral annulus calcification, with emphasis on its echocardiographic features. American heart journal. 1977; 94: 367-377.
- Mellino M, et al. Echographic-quantified severity of mitral anulus calcification: prognostic correlation to related hemodynamic, valvular, rhythm, and conduction abnormalities. American heart journal. 1982; 103: 222-225.
- Pomerance A. Pathology of the heart with and without cardiac failure in the aged. British heart journal. 1965; 27: 697.
- Benjamin EJ, et al. Mitral annular calcification and the risk of stroke in an elderly cohort. New England Journal of Medicine. 1992; 327: 374-379.
- Srivatsa SS, et al. Liquefaction Necrosis of Mitral Annular Calcification (LNMAC): Review of pathology, prevalence, imaging and management: Proposed diagnostic imaging criteria with detailed multi-modality and MRI image characterization. The international journal of cardiovascular imaging. 2012; 28: 1161- 1171.
- Salisbury AC, Shapiro BP, Martinez MW. Extensive myocardial and mitral annular calcification leading to mitral regurgitation and restrictive cardiomyopathy: An unusual case of caseous calcification of the mitral annulus. Journal of cardiovascular computed tomography. 2009; 3: 351-353.
- Bertrand PB, Mihos CG, Yucel E. Mitral annular calcification and calcific mitral stenosis: Therapeutic challenges and considerations. Current treatment options in cardiovascular medicine. 2019; 21: 1-12.
- Silbiger JJ, Anatomy, mechanics, and pathophysiology of the mitral annulus. American heart journal. 2012; 164: 163-176.
- Pressman GS, et al. Mitral annular dynamics in mitral annular calcification: A three-dimensional imaging study. Journal of the American Society of Echocardiography. 2015; 28: 786-794.
- Silbiger JJ, Bazaz R. Contemporary insights into the functional anatomy of the mitral valve. American heart journal. 2009; 158: 887-895.
- Fox E, et al. Epidemiology of mitral annular calcification and its predictive value for coronary events in African Americans: The Jackson Cohort of the Atherosclerotic Risk in Communities Study. American heart journal. 2004; 148: 979-984.
- Kanjanauthai S, et al. Relationships of mitral annular calcification to cardiovascular risk factors: The Multi-Ethnic Study of Atherosclerosis (MESA). Atherosclerosis. 2010; 213: 558-562.
- Boon A, et al. Cardiac valve calcification: Characteristics of patients with calcification of the mitral annulus or aortic valve. Heart. 1997; 78: 472-474.
- Elmariah S, et al. Risk factors associated with the incidence and progression of mitral annulus calcification: The multi-ethnic study of atherosclerosis. American heart journal. 2013; 166: 904-912.
- Roberts WC, Morphologic features of the normal and abnormal mitral valve. The American journal of cardiology. 1983; 51: 1005-1028.
- Sugihara N, Matsuzaki M. The influence of severe bone loss on mitral annular calcification in postmenopausal osteoporosis of elderly Japanese women. Japanese circulation journal. 1993; 57: 14-26.
- Waller BF, Roberts WC, Cardiovascular disease in the very elderly: Analysis of 40 necropsy patients aged 90 years or over. The American journal of cardiology. 1983; 51: 403-421.
- Abramowitz Y, et al. Mitral annulus calcification. Journal of the American College of Cardiology, 2015; 66: 1934-1941.
- Boon A, et al. Mitral annulus calcification is not an independent risk factor for stroke: A cohort study of 657 patients. Journal of neurology. 1997; 244: 535-541.
- Adler Y, et al. Mitral annulus calcification—a window to diffuse atherosclerosis of the vascular system. Atherosclerosis. 2001; 155: 1-8.
- Feindel CM, et al. Mitral valve surgery in patients with extensive calcification of the mitral annulus. The Journal of thoracic and cardiovascular surgery. 2003; 126: 777-781.
- Ben-Avi R, et al. Short-and long-term results after prosthetic mitral valve implantation in patients with severe mitral annulus calcification. Interactive cardiovascular and thoracic surgery. 2017; 24: 876-881.
- Ben-Avi R, et al. Short-and long-term results after prosthetic mitral valve implantation in patients with severe mitral annulus calcification. Interactive cardiovascular and thoracic surgery. 2017; 24: 876-881.
- Guerrero M, et al. Transcatheter mitral valve replacement in native mitral valve disease with severe mitral annular calcification: Results from the first multicenter global registry. JACC: Cardiovascular Interventions. 2016; 9: 1361-1371.
- Praz F, et al. Transatrial implantation of a transcatheter heart valve for severe mitral annular calcification. The Journal of thoracic and cardiovascular surgery. 2018; 156: 132-142.
- Maher E, et al. Aortic and mitral valve calcification in patients with end-stage renal disease. The Lancet. 1987; 330: 875-877.
- Urena M, et al. Current indications for transcatheter mitral valve replacement using transcatheter aortic valves: Valve-in-Valve, Valve-in-Ring, and Valve-in-Mitral annulus calcification. Circulation. 2021; 143: 178-196.
- You T, et al. Transcatheter mitral valve replacement for degenerated mitral valve bioprostheses, failure of mitral valvuloplasty and native valve with severe mitral annulus calcification: A systematic review and meta-analysis. Journal of cardiothoracic surgery. 2021; 16: 1-17.
- Urena M, et al. Causes and predictors of mortality after transcatheter mitral valve implantation in patients with severe mitral annulus calcification. Catheterization and Cardiovascular Interventions, 2021.
- Kato Y, et al. Association between mitral annulus calcification and subtypes of heart failure rehospitalization. Cardiology Journal, 2021.