
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Roseomonas gilardii bacteremia: A case report and literature review
Ali Hussain1*; Munawwar Hussain2; Upasana Aron1; Hassan Tahir3
1 Sentara Albemarle Medical Center Elizabeth City, North Carolina, USA.
2 UAMS Medical Center Little Rock, Arkansa, USA.
3 Lake Cumberland Regional Hospital Somerset, Kentucky, USA.
*Corresponding Author: Ali Hussain
Sentara Albemarle Medical Center Elizabeth City,
North Carolina, USA.
Email: Hussain.md@live.com
Received : Feb 15, 2022
Accepted : Mar 10, 2022
Published : Mar 17, 2022
Archived : www.jcimcr.org
Copyright : © Hussain A (2022).
Abstract
Bacteremia is a known complication of long-term central venous catheters and one of the most common reasons for removal. Usually, the infection happens after contamination from the skin during handling and rarely from the environmental organism. Roseomonas gilardii is a non-fermentative, oxidative Gram-negative coccobacillus. Roseomonas has been described in the literature as a rare opportunistic pathogen to cause bacteremia in the immunocompromised host. Herein, we report the case of a 67-year-old male who presented to ER with fever, nausea, and vomiting. He has been diagnosed with Roseomonas gilardii bacteremia from port infection in a small community hospital.
Citation: Hussain A, Hussain M, Aron U, Tahir H. Roseomonas gilardii bacteremia: A case report and literature review. J Clin Images Med Case Rep. 2022; 3(3): 1744.
Introduction
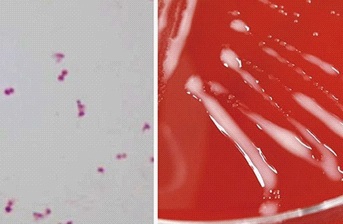
Roseomonas genus is pink pigmented, non-fermentative Gram-negative coccobacilli (Figure 1). Initially reported in the 1980s and used to be called pink coccoid groups [1]. Rihs et al. named genus Roseomonas in 1993 [2]. Infection in humans is not commonly reported, but Roseomonas has been isolated from blood associated with central venous catheters. The literature review also showed infrequent association with peritonitis, cellulitis, septic arthritis, and osteomyelitis [3-5]. Roseomonas usually have low pathological potential and mostly cause infection in immunocompromised individuals. Clinical significance of the organism is uncertain as Struthers et al. reviewed data of 35 patients, and only 60% of all the isolates were found to be associated with clinically significant primary or secondary infections [6]. Here we report a case of bacteremia likely associated with Medi port infection in a patient with colon cancer.
Case presentation
A 67-year-old black male presented to ER with a 2–3-day history of nausea and vomiting. On arrival in the ER, he had a fever of 101°F. Past medical history is significant for adenocarcinoma of the colon, on chemotherapy, status post colostomy, diabetes mellitus, and chronic kidney disease stage IIIb. The last dose of chemotherapy was three weeks ago. He did have diarrhea that is chronically present with a colostomy but no abdominal pain or any symptoms of urinary tract infection. The initial clinical exam in the ER was unremarkable. Blood workup showed leukocytosis of 14 K/uL, creatinine increased from baseline 2.7 to 3.4 mg/dL, and urine analysis showed 20-50/HPF RBC and 20-50/ HPF WBC. Blood cultures were obtained. The patient received sepsis treatment in the ER with intravenous fluids and antibiotics (Ceftriaxone), but he did not want to stay in the hospital and was discharged on oral antibiotics. Two days later, the patient presented with the same symptoms except that he was afebrile now. Leukocytosis 15.7 k/uL was present, and creatinine was even higher, 3.7 mg/dL now. He was started on intravenous fluids and admitted for acute kidney injury and dehydration. On day 5, 1 of his blood culture grew Gram-negative rods. We initiated Ceftriaxone 2 G every 24 hours. On day 7, the Gramnegative rods were identified as Roseomonas gilardii. Ceftriaxone was discontinued, and he was started on meropenem. No source of infection was identified except Medi Port, and we consulted Infectious disease for further recommendations. Repeat cultures were obtained and already showed no growth. During the hospitalization, the patient showed significant improvement in clinical status. His laboratory data also improved. He was on a regular diet, tolerated it well, and remained afebrile. Infectious Disease recommended a 14-day course of meropenem and did not recommend removing Medi port as the patient was already improved and repeat cultures showed no growth. After getting the midline, the patient was discharged home for a 14-day course of meropenem. On chart review after two weeks, the patient has completed antibiotics, his creatinine has improved, and back to his baseline functioning.
Discussion
Roseomonas is a rare pathogen, and clinical significance is unknown due to the rarity of the infections. Wang et al. studied 20 patients between 2000 and 2010 that had positive blood cultures with Roseomonas species. Catheter-related blood stream infection is one of the common presentations, and malignancy is as most frequent comorbid condition as reported in our case. They also concluded that the bacterium could cause infection in both adults and children irrespective of immune status [7]. Other common debilitating factors were chronic kidney disease, diabetes mellitus, ulcerative colitis, and cystic fibrosis. Most of the reported cases are opportunist infections, but in a retrospective review of 20 patients, 30% of the infections occurred in immunocompetent patients. Another feature of this organism is slow growth, which often takes 4-5 days to show positive blood cultures. Most of the reported data showed only 1 of the culture bottles showed any growth [6-8].
Dé et al. treated 36 patients with Roseomonas, and fever was the most common presenting symptom; 44% of infections were caused by more than one pathogen, and only 5 of these cases required removal of central venous catheter [9]. Our patient presented with fever, and at the end of treatment, we did not remove his Medi port due to improvement in his clinical condition and clearance of bloodstream infection. Our patient also had more than one pathogen in the only positive culture, and it was Gram-positive cocci which could not be isolated to identify.
The antibiotic susceptibility pattern of Roseomonas has been consistent with as reported in the literature. Rihs et al. tested the susceptibility of all 43 strains of bacterium against 26 different antibiotics, and only three antibiotics (amikacin, gentamycin, and imipenem) showed activity against all. Rihs also found that these strains were resistant to newer generation cephalosporins, cefotaxime, and ceftazidime [2]. Singal et al. are also reported resistance to trimethoprim/sulfamethoxazole, ceftazidime, and piperacillin/tazobactam and sensitivity to ceftriaxone, gentamicin, amikacin, doxycycline, ciprofloxacin, aztreonam, and meropenem [9]. We did not have data on antibiotic susceptibility, and we chose to treat our patient with meropenem as documented in most of the literature. Although the infections occur in the immunocompromised hosts, the mortality is relatively low, and most patients recover completely.
Conclusion
Roseomonas gilardii is a rare opportunistic pathogen that can cause true infection, mainly in immunocompromised individuals. This organism should be considered in Gram-negative septicemia in debilitated patients as a possible differential. Physicians should also consider the characteristics of R. gilardii due to its multi-drug resistant potential and slow to grow nature. This also highlights the importance of waiting for the final identification of organisms as well as susceptibility to antibiotics before discharging immunocompromised patients.
Disclosure
Conflict of interest/financial relationship: All authors have declared that there are noother relationships or activities that could appear to have influenced the submitted work
References
- Gilardi GL, Faur YC. Pseudomonas mesophilica and an unnamed taxon, clinical isolates of pink-pigmented oxidative bacteria. J Clin Microbiol. 1984; 20: 626-629.
- Rihs JD, Brenner DJ, Weaver RE, Steigerwalt AG, Hollis DG, Yu VL, et al. Roseomonas, a new genus associated with bacteremia and other human infections. J Clin Microbiol. 1993; 31: 3275-3283.
- Tsai SF, Chen CH, Shu KH, Wu MJ. Peritonitis caused by Roseomonas in a patient undergoing automated peritoneal dialysis: Case report and literature review. Intern Med. 2012; 51: 1721-1724.
- Shokar NK, Shokar GS, Islam J, Cass AR. Roseomonas gilardii infection: Case report and review. J Clin Microbiol. 2002; 40: 4789- 4791.
- Fanella S, Schantz D, Karlowsky J, Rubinstein E. Septic arthritis due to Roseomonas gilardii in an immunocompetent adolescent. J Med Microbiol. 2009; 58: 1514-1516.
- Struthers M, Wong J, Janda JM. An initial appraisal of the clinical significance of Roseomonas species associated with human infections. Clin Infect Dis. 1996; 23: 729-733.
- Ching-Min Wang, Chih-Cheng Lai, Che-Kim Tan, Yu-Chuang Huang, Kuei-Pin Chung, et al. Clinical characteristics of infections caused by Roseomonas species and antimicrobial susceptibilities of the isolates. 2012; 72: 0–203.
- Indra Dé, Rolston KVI, Han XY. Clinical Significance of Roseomonas Species Isolated from Catheter and Blood Samples: Analysis of 36 Cases in Patients with Cancer, Clinical Infectious Diseases. 2004; 38: 1579–1584. https://doi.org/10.1086/420824
- Singal A, Malani PN, Day LJ, Pagani FD, Clark NM. Roseomonas infection associated with a left ventricular assist device. Infect Control Hosp Epidemiol. 2003; 24: 963-965.