
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A rare bird spotted: Inferior vena cava-calyceal fistula on pelvic kidney following on iatrogenic injury during a retrograde intrarenal surgery
Adil Mellouki1,2; Arnoult Morrone2; Romain Haider2; Daniel Chevallier2; Youness Ahallal2; Matthieu Durand2
1 Department of Urology, Andrology and Renal Transplant, Hassan II University Hospital, Fez, Morocco
2 Department of Urology, Andrology and Renal Transplant, Pasteur II University Hospital, Nice, France.
*Corresponding Author: Adil Mellouki
Department of Urology, Andrology and Renal Transplant, Hassan II University Hospital, Fez, Morocco.
Email: [email protected]
Received : Feb 12, 2022
Accepted : Mar 10, 2022
Published : Mar 17, 2022
Archived : www.jcimcr.org
Copyright : © Mellouki A (2022).
Abstract
We report the case of an 18-year old woman presenting an inferior vena cava-calyceal fistula on a pelvic kidney revealed by chronic pelvic pain and recurrent pyelonephritis 6 months following an iatrogenic renal injury during an ureterscopy for renal stone.
Retrograde ureteropyelography imaging showed a fistula between the upper calix and the inferior vena cava. First, the fistula was treated by open surgery, due to the recurrence, a total nephrectomy was necessary. We aims to emphasis an exceptionally rare surgical complication of ureteroscopy, as well as the treatment options.
Citation: Mellouk A, Morrone A, Haider R, Chevallier D, Ahallal Y, et al. A rare bird spotted: Inferior Vena cava-calyceal fistula on pelvic kidney following an iatrogenic injury during a retrograde intrarenal surgery. J Clin Images Med Case Rep. 2022; 3(3): 1745.
Introduction
Calico-Venous Fistula (FCV) is an abnormal communication between the pyelo-caliciel urinary collecting system and the venous system.
The clinical presentation is variable, associating pain, macroscopic hematuria, renal colic or even pyelonephritis.
FCVs are very rare surgical complications following major procedures such as kidney transplantation, percutaneous nephrolithotomy, chronic ureteral obstruction or of iatrogenic origin [1].
Our objective is to describe this rare and morbid complication through a clinical case as well as the different possibilities of its treatment.
Case presentation
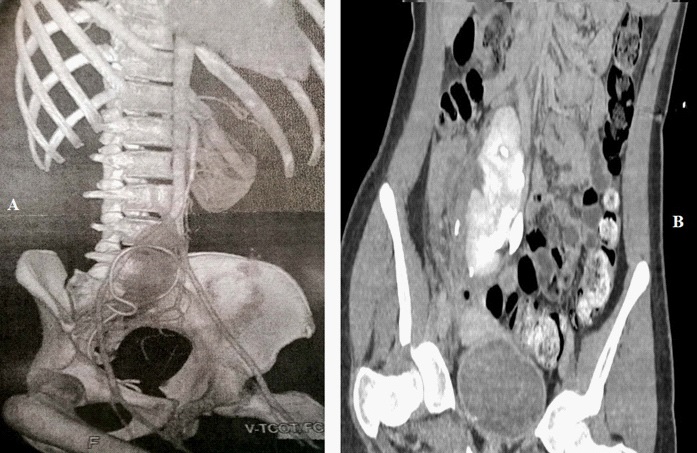
A young 17-year-old girl patient with a urological malformation (a right pelvic kidney) presenting an 8 mm lithiasis in her pelvic kidney treated by endoscopic Retrograde Intrarenal Surgery (RIRS) and placement of a JJ stent. At 72 hours of the procedure she consults the emergency department for acute pelvic pain. The CT scan performed reports an endoureteral stent transfixing the right pelvic kidney at the level of the superior calyx with perirenal hematoma. It was treated by repositioning the JJ stent and active surveillance (Figure 1).
At D7 post RIRS she presented for pyelonephritis, the CT scan performed found multiple foci of nephritis, a 50 X 30 X 90 mm uro-hematoma fed by leakage from the upper calyx imposing radiological drainage (Figure 1).
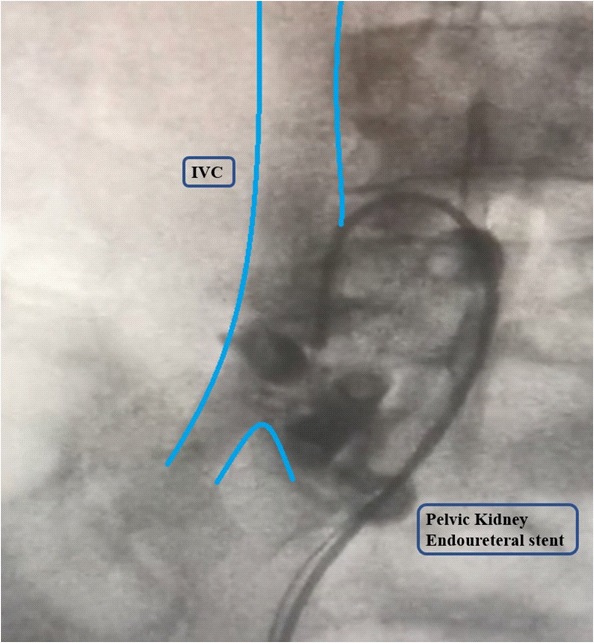
For 6 months a series of hospitalizations for different reasons: pyelonephritis, renal colic, pain on JJ stent without any imaging being able to demonstrate an organic cause for pain requiring multimodal analgesia, this justified the performance of an RIRS with a diagnostic retrograde ureteropyelography, which found a calico-venous fistula (Figure 2).
A few days later, the patient presented with significant macroscopic hematuria. A double team (urologists and vascular surgeons) open surgery was performed for fistula treatment. The surgical exploration allows the demonstration of the fistulous zone between a collateral vein of the right renal vein at the origin of the IVC and the superior calix of the right pelvic kidney allowing the section of this collateral after ligation of both sides. At the end of the procedure, a radiological control by UPR is carried out.
Regarding psychosocial aspect, there was a significant impact with depression, isolation and interruption of schooling, requiring sustained psychosocial supervision.
The patient faced recurrent pelvic pain, repeated hospitalizations, and the interruption of her educational program despite the fistula treatment, we retain a recurrence of the fistula confirmed by retrograde ureteropyelography with indication of simple right pelvic nephrectomy by open surgery after parental consent.
At the D1, there was no complications, the patient is discharged at D3, she remained asymptomatic during the followup at 1 and 6 months postoperatively with normal renal function.
Discussion
During acute ureteral obstruction, renal backflow brings together 5 urine reabsorption mechanisms that allow urinary secretion: pyelovenous, pyelo-lymphatic, pyelo-tubular, pyelo-interstitial and pyelo-sinus [2]. The hyperpressure induced during UPR ease the visualization of these reabsorption mechanisms. Chronic ureteral obstruction can therefore in some cases result in the formation of a fistula by rupture of the fornix in the venous system.
In the literature, the majority of cases of FCV are due to a chronic obstruction, in our case the fistula has an iatrogenic origin. The treatments for calico-venous fistulas described in the literature are based on selective embolization and surgery ranging from elective fistula repair, partial nephrectomy or even total nephrectomy [3,4].
Venyo and Shah reported the success of selective embolization in the setting of a right pyelo-venous fistula between the pelvis and a tortuous inferior polar vein diagnosed during an intermittent macroscopic hematuria work-up [4].
In our case, no non-invasive imaging was able to formally identify the fistula which was unmasked by the hypertension induced during the diagnostic UPR, a condition which is difficult to achieve by other imaging exam. To this, is added the pelvic position of the right kidney.
Surgery would be indicated as a second line treatment, first with partial nephrectomy if the fistula is clearly individualized on preoperative imaging without association of venous thrombosis, then finally with total nephrectomy in the situation of treatment failure or venous thrombosis or hemodynamic instability [3,4].
After failure of the fistula repair, partial nephrectomy appears difficult to perform in such an inflammatory environment and the pelvic kidney position, hence the choice of our therapeutic altitude by total nephrectomy.
Conclusion
Through our case report, we aims to emphasis an exceptionally rare surgical complication of endoscopic retrograde intrarenal surgery in a pelvic kidney, as well as the treatment options.
The therapeutic strategy must be the least invasive possible and be based on selective embolization and surgery ranging from elective fistula repair, partial nephrectomy or even total nephrectomy
Declarations
Consent: Written informed consent has been obtained by the patient.
Conflicts of interests: There are no conflicts of interest among the authors to disclose.
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-forprofit sectors.
Acknowledgements: None.
References
- Nemeth AJ, Patel SK. Pyelovenous backflow seen on CT urography. Am J Roentgenol. 2004; 182: 532–533.
- Low L, Devcich A. Calyceal-venous fistula of the kidney: A rare case report and review of literature. Urology case reports. 2019; 23 : 23-24
- Venyo AK, Shah S. Lower polar aberrant renal vein – renal pelvis fistula: A rare cause of Haematuria. W Afr J Med. 2008; 27: 267- 270.
- Turki MA, Onuora VC, Koko AH, et al. Pyelovenous fistula: An uncommon cause of ‘Essential Haematuria’. Urol Int. 1998; 60: 189-190.