
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Role of magnetic resonance imaging in the pre‐surgical planning of perianal hidradenitis suppurativa, complicated by anal fistulae: A case report and review of the literature
Pier Paolo Arcuri1*; Laura Comito2; Barbara Vavalà1; Domenico Laganà2
1 Radiology Unit, Department of Radiology, Pugliese-Ciaccio Hospital, Catanzaro, Italy
2 Radiology Unit, Department of Experimental and Clinical Medicine, “Magna Graecia” University, Catanzaro, Italy
*Corresponding Author: Pier Paolo Arcuri
Radiology Unit, Department of Radiology, PuglieseCiaccio Hospital, Catanzaro, Italy.
Email: pierpaoloarcuri@unicz.it
Received : Feb 16, 2022
Accepted : Mar 11, 2022
Published : Mar 18, 2022
Archived : www.jcimcr.org
Copyright : © Arcuri PP (2022).
Abstract
Hidradenitis Suppurativa (HS) is a chronic inflammatory disease of the skin starting from the apocrine glands and mainly involving the axilla, perineum and perianal area. It is clinically defined by the onset of painful subcutaneous nodularities, associated with signs of local inflammation, whose progression proceeds towards the definition of true subcutaneous abscess collections from which fistulous pathways branch off. These lesions result in severe fibro-cicatricial deformities.
The diagnosis of HS, which is basically clinical, is followed, due to the recurrent/relapsed nature of the disease, by a difficult therapeutic management, which makes use of different treatments depending on the severity of the pathological picture, ranging from topical or systemic medical therapy to surgical excision.
Imaging examinations, although not specific enough in the diagnosis of HS, are essential to define the loco-regional extension of the disease and to exclude possible alternative diagnoses. In particular, MRI plays a key role in the study of HS with anogenital localization, both for the recognition of lesions in the active phase and for the assessment of the local extension of the disease, in particular in adequately demonstrating the entire course of the fistulas and the relationships with the neighboring anatomical structures. This allows the optimization of its treatment, in order to reduce disease recurrence. The case presented by us describes the MRI characteristics in a rare case of HS, complicated by anal fistulae.
Keywords: Hidradenitis suppurativa (HS); Crohn’s disease; Magnetic resonace imaging.
Citation: Arcuri PP, Comito L, Vavalà B, Laganà D. Role of magnetic resonance imaging in the pre‐surgical planning of perianal hidradenitis suppurativa, complicated by anal fistulae: A case report and review of the literature. J Clin Images Med Case Rep. 2022; 3(3): 1746.
Introduction
Hidradenitis Suppurativa (HS) is defined as a chronic and disabling skin disorder affecting the pilo-sebaceous units of skin regions rich in apocrine sweat glands. It is characterized by occlusion and subsequent acneiform follicular inflammation and relapsing muco-purulent infections, with progressive formation of dermo-hypodermic abscess collections and fistulous pathways leading to local scar deformities [1].
The diagnosis of HS is essentially clinical, but imaging examinations play an important complementary role in both the early and advanced stages of the disease, allowing, in particular MRI [2], the recognition of lesions in the active phase, the assessment of the local extension of the disease and the identification of possible complications. In fact, the anal sphincter region cannot be visualised by fistulography and, therefore, its possible involvement cannot be detected. CT scans, due to their low contrast resolution, can scarcely define the presence of inflammatory striae in the soft tissue area. Endorectal ultrasound is not suitable for detecting involvement of supra- and extra-sphincteric tissues. On the other hand, MRI, thanks to its intrinsic high contrast resolution and multiplanarity, is able to adequately demonstrate the entire course of the fistulae and the relationships with neighbouring anatomical structures.
HS is a pathology with a variable evolution and a difficult therapeutic management; the latter varies from the use of local and/or systemic pharmacological therapies to surgical excision [3].
In the case presented here, we highlight the impact of MRI in the correct definition of the fistulous features associated with the disease and, therefore, the correct diagnostic and pre-surgical classification.
Presentation of case
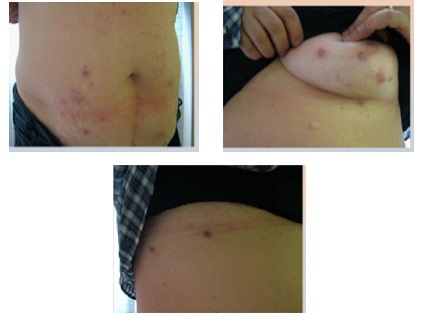
A 56-year-old woman with a remote pathological history (about 15 years previously) of Crohn’s disease presented with vaginal burning sensation and recent appearance of multiple purulent lesions, first in the groin and then on the hips and trunk (Figure 1a,1b,1c).
When a perineal abscess formation was suspected, in relation to her history of Crohn’s disease, she underwent pelvic MRI performed with 1.5 T magnet strenght, in basal conditions and subsequently to Intravenous (i.v.) administration of paramagnetic contrast medium, with T1w spin-echo, T2w fast spin-echo, STIR and SPIR sequences (with saturation of adipose tissue).
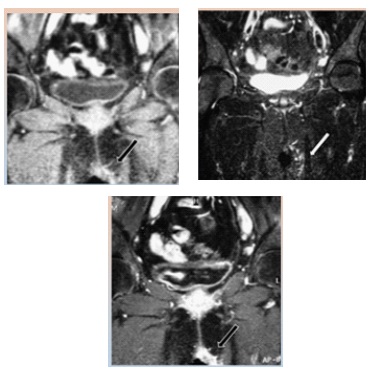
The MRI examination reveals considerable thickening of the skin and hardening of the subcutaneous tissues in the left median/paramedian region of the vulva and the proximal part of the vagina, characterized by low signal intensity in the T1-weighted sequence (Figure 2a) and high signal intensity in the STIR sequence (Figure 2b), which, after i.v. of Mdc, shows significant contrast enhancement (Figure 2c).
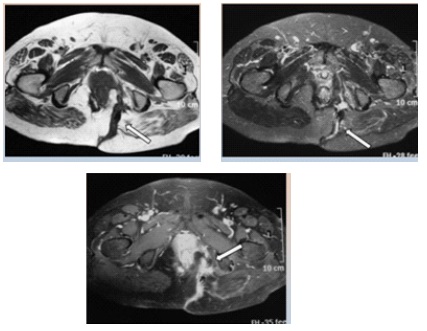
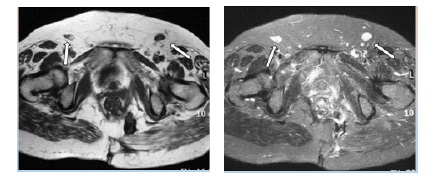
In association with the subcutaneous planes, multiple small hypointense areolas in T1w and hyperintense areolas in T2w and STIR are found (Figure 3a,3b), characterised by “inhomogeneous enhancement” in the post-contrastographic sequences: characteristics compatible with small abscess collections (Figure 3c).
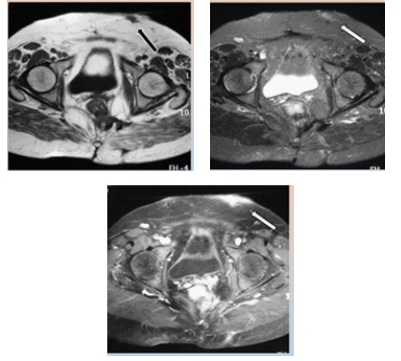
These abscesses, located at a distance from both the rectum and the anus, have no communication link with the bladder, urethral and rectal walls (Figure 4a,4b,4c).
Increased lymph nodes are found in the bilateral inguinal area (Figure 5a, 5b).
On the basis of the clinical history and radiological features, the lesions are not indicative of a perianal localisation of Crohn’s disease, but rather point to a form of suppurative hydroxyadenitis with ano-perineal involvement.
In order to obtain a diagnosis of certainty, the patient undergoes biopsy and histological examination of the pathological tissue, which confirms the radiological diagnosis. On the basis of the information obtained from the MRI examination, in particular regarding the fistulous pathways and their relationship with the neighbouring structures, the patient undergoes surgery.
Discussion
First described by Velpeau in 1839 [4] and subsequently by Verneuil in 1864 [5], Hidradenitis Suppurativa (HS), also known as Verneuil’s disease or acne inversa, is a chronic and recurrent inflammatory skin disorder characterized by the appearance of erythematous and painful nodules in the deep subcutaneous planes. These nodularities, hard in the initial phase and then progressing to a soft consistency, in relation to internal suppuration phenomena, may evolve towards the formation of abscess collections and fistulas [6,7].
Although considered a rare condition, HS affects 1 to 4% of the world’s population, most commonly during the second and third decades of life, with a clear prevalence for the female sex (3.3F: 1M) [6,8-11].
With an as yet unknown aetiology, probably related to excessive sweating and heat, the use of tight-fitting clothing and deodorants, and depilation, HS is thought to be the result of occlusion of the apocrine duct of hair follicles by a keratin plug, with initial follicular infection and formation of an abscess nodule, the possible subsequent rupture of which triggers an extensive inflammatory process and results in a dermo-hypodermic [12-14] abscess collection (sinus tract) that will result in scarring and local deformities.
In relation to the aforementioned pathogenesis, it is clear that HS is localised in the intertriginous areas of the body rich in apocrine glands (axillary, inguinal, perineal and perianal, mammary and inframammary, gluteal and retro-auricular regions), with a higher frequency in the infra-ammary (23%) and inguinal (93%) regions in women and in the gluteal (40%) and peri-anal (51%) regions in men [6].
Peri-anal HS is the form of HS originating from the apocrine glands located in the skin and soft tissues adjacent to the anus. It occurs in approximately 32% of patients with HS and appears to be associated with more disabling [6,15] outcomes and, as previously mentioned, is more common in males [6]. It is frequently associated with other pathological [15] conditions, and in particular a significant association has been found with Crohn’s disease, which is present in approximately 38% of cases [16-19].
The diagnosis of HS is essentially clinical (typical recurrent skin lesions: painful and malodorous nodules, abscess collections and scarring) and biopsy examination for diagnostic confirmation is very rarely performed [20].
Evaluation by imaging methods, although not specific enough for diagnostic definition, is of utmost utility for quantification of the extent of disease, for exclusion of possible alternative/differential diagnoses and for proper surgical planning [3].
In fact, the assessment of disease severity based on clinical data alone has some limitations. The clinical interpretation of the local spatial extension of the disease based on the palpatory evaluation of the lesions, in fact, is limited due to the concomitant presence of an intense inflammatory process in the tissues involved, which, in addition to masking the extent of the pathological process, could also determine an incorrect distinction between a nodular lesion and a fistula, conditioning an erroneous staging of the disease and consequent therapeutic choice [21].
Thus, the role of imaging is to define the type and extent of lesions in HS, confirming the diagnosis and providing objective and accurate information, and the degree of severity of the disease, and in therapeutic monitoring and/or surgical planning.
It has been noted that clinical evaluation alone tends to significantly underestimate the severity of the disease compared to US [21,22] examination, and that surgical treatment would benefit significantly from an accurate pre-operative assessment of the degree of loco-regional disease extension, since recurrence of the pathological picture due to inadequate surgical radicality represents a significant problem in approximately 13- 27% of cases [23].
The first level imaging examination for the assessment of HS is the ultrasound examination supplemented by the colourdoppler technique, which can guarantee the study of the skin and its underlying layers with good resolution [24].
MRI, on the other hand, is mainly performed in cases of HS with predominantly and/or exclusively ano-genital localisation [25].
More specifically, MRI examination of the pelvis, as in the case previously described, allows the diagnosis to be confirmed, ensuring the differential diagnosis with respect to other pathological conditions, in particular perianal disease from Crohn’s disease, and defining a balance of disease extension.
In the course of perianal HS, on MRI examination there is a thickening of the dermis and subcutaneous planes, corresponding to an area of the subcutaneous planes with clear-cut borders, characterized by low signal in T1w sequences, high signal in T2w sequences and signal restriction in diffusion-weighted sequences, which after i.v. administration of paramagnetic contrast medium presents a significant contrastographic enhancement. The above alteration is frequently associated with the presence of abscess collections in the context of subcutaneous tissues, identifiable as hypointense areolae in T1-weighted sequences and hyperintense in T2-weighted sequences with peripheral contrast enhancement after administration of mdc. In the most severe cases, a fistulous passage is also recognisable, which from the abscessal and confluent collections of the subcutaneous tissue heads to the surface, draining into the skin layers or externally, or in some cases reaches the wall of the distal third of the rectum or the analcanal [26].
Considering the typical MRI features described above, it is clear that making the differential diagnosis between perianal HS and Crohn’s disease is a real diagnostic challenge, both because both diseases can present with the same tissue changes and because it is not uncommon for the two diseases to coexist, with signs of one overlapping with those of the other [27-29].
The MRI features to be considered/analysed to make the differential diagnosis between perianal HS and ano-perineal disease in Crohn’s are the site, distribution and characteristics of the lesions and associated signs of disease.
In particular, according to a review of the data available in the literature conducted by Monnier et all. [20], in perianal HS the lesions are more frequently located in the inguinal area anteriorly, along the intergluteal fold and in the sacral/gluteal area posteriorly, in the absence of a prevalent perianallocation [25,30] and show bilateral involvement of the above areas.
With regard to the type of lesion, it has been shown that inflammatory granulomas are found more frequently and statistically significantly in patients with HS. Abscesses, on the other hand, occur without clear specificity in both pathological pictures, although in HS they are more numerous and tend to confluence [20]. Finally, fistulous tracts seem to be more frequent in patients with Crohn’s disease than in those with HS, whose communication with the anal canal is rare [20].
In patients with HS the lesions are characteristically associated with diffuse subcutaneous oedema, rather than the thickening of the rectal wall typical of Crohn’s disease.
Thus, in summary, the finding of typical lesions (abscesses, inflammatory granulomas, fistulous tracts) in the inguinal, intergluteal and sacral/gluteal regions with bilateral involvement and associated with diffuse oedema of the subcutaneous tissue supports the diagnosis of perianal HS.
The correct diagnostic classification of perianal HS rather than Crohn’s disease is important, particularly in cases where the two conditions coexist, for the correct therapeutic management of the disease. In cases related to HS, in fact, the treatment involves a combination of antibiotic and biological drugs, but also hormone therapy, zinc and retinoids in association with specific dermatological treatments, such as ablation by CO2 laser or radiofrequency [6]. In Crohn’s disease, on the other hand, combinations of antibiotics, immunomodulants and anti-TNF drugs are used.
Conclusions
In conclusion, with this work on HS, a pathology that is often misunderstood and consequently misdiagnosed by radiologists, we wanted to spread the knowledge and underline the important role that imaging plays in this pathology, since it conditions the correct diagnostic classification, especially for forms with perianal localization that are difficult to differentiate, and therapeutic and radicality of a possible surgical treatment.
This desire stems from the consideration that correct diagnosis and management of the disease would have a significant impact on a pathology which, despite being considered rare, is, of all skin diseases, the one associated with the highest morbidity and lowest quality of life [31].
Indeed, the quality of life of patients with HS is severely compromised in relation to the pain, bad odour and high recurrence of symptoms associated with the disease, as well as the fibro-cicatricial outcomes of the disease itself or its surgical treatment [32,33].
In the field of imaging methods, MRI plays a decisive role, given the high contrast resolution and multiplanarity, intrinsic characteristics of the method, in precisely defining the course of the fistulous traps as well as the relationships with the sphincters, essential information for a correct differential diagnosis and adequate surgical planning, as in the case presented here. The images obtained post Gadolinium have better highlighted, through enhancement, the walls of the abscesses and the fistulous tramites. Due to the high cost and limited ability to detect small superficial lesions, MR imaging is suggested, primarily in the pre-surgical planning of extensive cases of HS.
Declarations
Conflict of interest: The authors disclosure of any personal or financial support or author involvement with organization with financial interest in the subject matter or any actual or po¬tential conflict of interest.
Acknowledgements: special thanks to Andrea Teodoro Ra¬diographer.
References
- Poh F, Wong SK. Imaging of hidradenitis suppurativa and its complications. Case Rep Radiol. 2014; 2014: 294753.
- Hirotoshi Takiyama, Shinsuke Kazama, Yusuke Tanoue et all. Efficacy of magnetic resonance imaging in the diagnosis of perianal hidradenitis suppurativa, complicated by anal fistulae: A report of two cases and review of the literature. Int J Surg Case Rep. 2015; 15: 107-111.
- Lopes AA, Moraes GN, Dias BMML, Souza GD, Souza LQ. Preoperative imaging assessment of hidradenitis suppurativa. Rev. Bras. Cir.Plást. 2019; 34: 264-267.
- Velpeau A. Dictionnare de Medicine, un Repertoire Genenral Des Sciences Medicales Sous La Rapport Therorique et Practique; 1839.
- Verneuil A. Etudes sur les tumeurs de la peau: De quelques maladies des glandes sudoripares. Arch Gen Med. 1854; 2: 447-468.
- Alikhan A, Lynch PJ, Eisen DB. Hidradenitis suppurativa: A comprehensive review. J Am Acad Dermatol 2009; 60:539-561.
- Jansen I, Altmeyer P, Piewig G. Acne inversa (aka hidradenitis suppurativa). J Eur Acad Dermatol Venereol 2001; 15: 532-540.
- Cosmatos I, Matcho A, Weinstein R. Analysis of patient claims data to determine the prevalence of hidradenitis suppurativa in the United States. J Am Acad Dermatol. 2013; 68: 412-419.
- Cosmatos I, Matcho A, Weinstein R. Analysis of patient claims data to determine the prevalence of hidradenitis suppurativa in the United States. J Am Acad Dermatol. 2013; 68: 412-419.
- Jemec GBE. Hidradenitis suppurativa. N Engl J Med. 2012; 366: 158-164.
- McMillan K. Hidradenitis suppurativa: Number of diagnosed patients, demographic characteristics, and treatment patterns in the United States. Am J Epidemiol. 2014; 179: 1477-1483.
- Graham PM. The Boils Below: Hidradenitis Suppurativa. drpmg. com/2016/08/25/the-boils-below-hidra denitis suppurativa. 2016.
- Napolitano M, Megna M, et al. Hidradenitis suppurativa: from pathogenesis to diagnosis and treatment. Clin Cosmet Investig Dermatol. 2017; 10: 105.
- Saunte D, Jemec G. Hidradenitis Suppurativa: advances in diagnosis and treatment. JAMA. 2017; 318: 2019‐2032.
- Dessinioti C, Katsambas A, Antoniou C. Hidradenitis suppurrativa (acne inversa) as a systemic disease. Clin Dermatol. 2014; 32: 397-408.
- Dambha F, Tanner J, Carroll N. Diagnostic imaging in Crohn’s disease: What is the new gold standard? Best Pract Res Clin Gastroenterol. 2014; 28: 421-436.
- Dambha F, Tanner J, Carroll N. Diagnostic imaging in Crohn’s disease: What is the new gold standard? Best Pract Res Clin Gastroenterol. 2014; 28: 421-436.
- Taylor SA, Halligan S, Bartram CI. Pilonidal sinus disease: MR imaging distinction from fistula in anus. Radiology. 2003; 226: 662- 667.
- Taylor SA, Avni F, Cronin CG et al. The first joint ESGAR/ESPR consensus statement on the technical performance of crosssectional small bowel and colonic imaging. Eur Radiol. 2016.
- Monnier L, Dohan A, Amara N et al. Anoperineal disease in Hidradenitis Suppurativa: MR imaging distinction from perianal Crohn’s disease. Eur Radiol. 2017; 27: 4100-4109.
- Wortsman X, Moreno C, Soto R, et al. Ultrasound in-depth characterization and staging of hidradenitis suppurativa. Dermatol Surg. 2013; 39: 1835-1842.
- Napolitano M, Calzavara-Pinton PG, Zanca A, et al. Comparison of clinical and ultrasound scores in patients with hidradenitis suppurativa: Results from an Italian ultrasound working group. J Eur Acad Dermatol Venereol. 2019; 33: e84-e87.
- Mehdizadeh A, Hazen PG, Bechara FG, et al. Recurrence of hidradenitis suppurativa after surgical management: a systematic review and meta-analysis. J Am Acad Dermatol. 2015; 73: S70- S77.
- Wortsman X, Wortsman J. Clinical usefulness of variable frequency ultrasound in localized lesions of the skin. J Am Acad Dermatol. 2010; 62: 247-256.
- Griffin N, Williams AB, Anderson S, et al. Hidradenitis suppurativa: MRI features in anogenital disease. Dis Colon Rectum. 2014; 57: 762-771.
- Montaña N, Labra A, Panussis D. Hidradenitis supurativa, evaluación por resonancia magnética. Rev Chil Radiol. 2014; 20: 159- 163.
- Yazdanyar S, Miller IM, Jemec GB. Hidradenitis suppurativa and Crohn’s disease: two cases that support an association. Acta Dermatovenerol Alp Pannonica Adriat. 2010; 19: 23-25.
- Van der Zee HH, van derWoude CJ, Florencia EF, Prens EP. Hidradenitis suppurativa and inflammatory bowel disease: are they associated? Results of a pilot study. Br J Dermatol. 2010; 162: 195-197.
- Church JM, Fazio VW, Lavery IC, Oakley JR, Milsom JW. The differential diagnosis and comorbidity of hidradenitis suppurativa and perianal Crohn’s disease. Int J Color Dis. 1993; 8: 117-119.
- Kelly AM, Cronin P. MRI features of hidradenitis suppurativa and review of the literature. AJR Am J Roentgenol. 2005; 185: 201- 1204.
- Von der Werth J, Jemec G. Morbidity in patients with hidradenitis suppurativa. Br J Dermatol. 2001; 144: 809-813.
- Slade DE, Powell BW, Mortimer PS. Hidradenitis Suppurativa: Pathogenesis and management. Br J Plast Surg 2003; 56: 451- 461.
- Asgeirsson T, Nunoo R, Luchtefeld MA. Hidradenitis Suppurativa and Pruritus Ani. Clin Colon Rectal Surg. 2011; 24: 71-80.