
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Analysis of clinical characteristics of subacute combined degeneration on three cases of delayed diagnosis
Anqi Tang1; Tan Li1; Qianqian Ding2; Zhi Wang1; Yuan Liu3*; Xiuying Cai1*
1 Department of Neurology, The First Affiliated Hospital of Soochow University, 899 Pinghai Road, Suzhou, Jiangsu 215006, China.
2 Department of Neurology, Suzhou Wuzhong People’s Hospital, 61 Dongwu North Road, Suzhou, Jiangsu 215128, China.
3 Department of Neurology, Suzhou Ninth People’s Hospital, 2688 Ludang Road, Suzhou, Jiangsu, 215200, China.
*Corresponding Author: Xiuying Cai
Department of Neurology, The First Affiliated Hospital of Soo Chow University, Suzhou, Jiangsu, China.
Email: cxy9990888@163.com
Received : Feb 18, 2022
Accepted : Mar 14, 2022
Published : Mar 21, 2022
Archived : www.jcimcr.org
Copyright : © Cai X & Liu Y (2022).
Abstract
Purpose: Subacute Combined Degeneration (SCD) is a kind of neurodegenerative diseases which is easy to be misdiagnosed because of some promiscuous symptoms and atypical laboratory test results. The prognosis would be poor if patients had clinical symptoms of myelopathy for a long time. Therefore, doctors should combine pre-existing conditions, clinical symptoms and correlated laboratory examinations to make definite diagnosis quickly and accurately.
Case report: Three middle-aged patients aged from 41 to 63, one male and two females were diagnosed SCD with progressive ascending numbness in four limbs or both legs. For some reason, none of them got the right diagnosis in the first place. In case 1, blood cell analysis revealed a decrease in three series including white blood cells, platelets and hemoglobin. In case 2, the blood cell analysis of the patient did not show signs of anemia at all. While the initial clinical symptom in case 3 was just a mild psychiatric symptom. Although their final diagnosis were clear, the failure not to take SCD into consideration at the first time was worthy of reflection. Fortunately, their neurological status improved after vitamin B12 supplementation.
Conclusion: Usually, some confusing symptoms and a typical laboratory may make SCD easy to be misdiagnosed. Early diagnosis and treatment are critical to the prognosis. Thus, the clinicians must capture the related clinical characteristics.
Keywords: subacute combined degeneration; vitamin b12 deficiency; clinical characteristics.
Citation: Tang A, Li T, Ding Q, Liu Y, Cai X, et al. Analysis of clinical characteristics of subacute combined degeneration in three cases of delayed diagnosis. J Clin Images Med Case Rep. 2022; 3(3): 1748.
Introduction
Subacute Combined Degeneration (SCD) is a kind of degenerative disease referring to the injury of posterior and lateral columns of the spinal cord, which is usually induced by Vitamin B12 deficiency. The cardinal symptoms of SCD were paresthesia, ataxia, instability of gait, spastic paraplegia, and peripheral neuropathy. Vitamin B12 deficiency can result in body disorders in lots of systems, such as hematological, digestive, mental and central nervous systems [1]. The clinical characteristics of SCD may not be typical, for instance, the gastric diseases may be absent, the disorder in hematological system may not exist, besides, some patients even have the separate symptom of mental anomaly. Early identification and treatment are urgent and significant for SCD, which will protect patients from irreversible neurological sequelae. Therefore, how the clinicians capture the effective clues to make the right diagnosis is worth discussing.
Here, we report on three patients who were diagnosed SCD with progressive ascending numbness in four limbs or both legs, but for some reason, none of them got the right diagnosis in the first place.
Case presentations
Case 1
The patient was a 63-year-old retired woman living in China with a personal history of hypertension and chronic gastroenteritis. Her diet was varied.
One week ago before she came to our hospital, she began to feel numbness and weakness in her lower extremities, sustaining free from the rest or exercise. The abnormalities were not paid attention at first. Shortly afterwards, she had the symptom of ataxia. She did not come to the hospital until she lost the ability of independent ambulation.
Based on the past medical history, we found that the patient had suffered from glottitis for almost five years, and had no response to treatment of medications. She had poor appetite two weeks ago. She didn’t receive any blood test during such a long time except gastroscope examination.
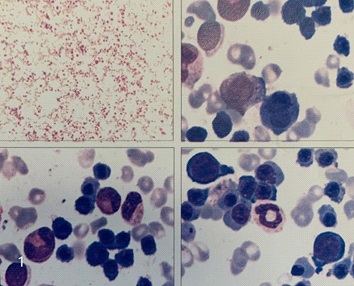
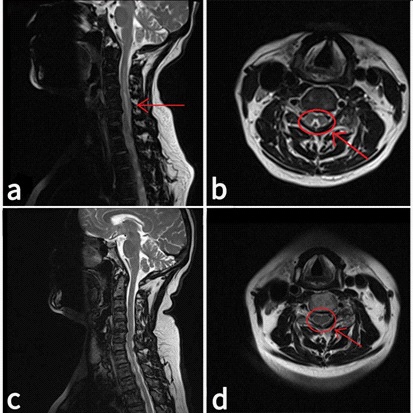
On admission, neurological examination revealed that the mental status, cranial nerve and the strength of all limbs are normal. Her mirror-like tongue was notable. Besides, she also had hypesthesia in arms and legs. We also observed absent knee and achilles jerk as well as negative babinski reflex in the neurological examination. The routine blood examination shocked us. The results revealed a decrease in white blood cells, platelets and hemoglobin (WBC 2.56 X 109 /L, PLT 100 X 109 /L, HGB 64g/L, MCV 107.0fl). Thyroid function, Paroxysmal Hemoglobinuria (PNH) test, Myelodysplastic Syndrome (MDS) immunologic test, multiple PCR test and Nerve Conduction Velocity (NCV) test were all normal. Significantly, Vitamin B12 concentration was 10 pg/ml (180-914), while the folate concentration was 24 ng/ml (3.1-19.9). We even did bone marrow puncture for further examination, the result showed hyperplasia of the bone marrow with a decreased erythroid ratio and megaloblastic-like changes could be observed (Figure 1). TET2 gene p.Gln705* and KMT2C gene p.Pro821Leu mutation were detected. These specialized examinations were of great benefit for us to distinguish the disease from refractory anemia. Furthermore, the patient also received whole spine MRI scan. The MRI demonstrated normal T1 and high T2 signal in the posterior and lateral columns from C3-T11 level (Figure 2a), while axial T2-weighted imaging showed high signal vividly described as a inverted V sign [2-4] (Figure 2b).
The patient received a dose of vitamin B12 0.5 mg/d and vitamin B1 100 mg/d via intramuscular injection and folic acid tablets 5 mg/d through the mouth. After two weeks of treatment, she could independently maintain a standing position with a walker, but she still had difficulty in walking by herself. The paresthesia in the lower extremities improved substantially. After discharged from the hospital, she was treated by oral administration of vitamin B12 500 μg three times a day and folic acid tablets 5 mg/d. Physical therapy focusing on activities of daily living continued.
Four months later after discharge, she came to our clinic for return visit. She was able to walk alone without any help, though the numbness in her right lower extremity still haunted her. Blood tests as well as vitamin B12 concentration were normal. We also reviewed the cervical cord magnetic resonance, the abnormal signal disappeared (Figure 2c,d).
Case 2
A 41-year-old male suffered from persistent numbness in his ring and middle fingers for two months. He was a factory worker. He had drunk two liquors a day for ten years. He went to the local hospital for MRI examination of his cervical spine, the results was abnormal. He was then referred to our neurology ward for further treatment.
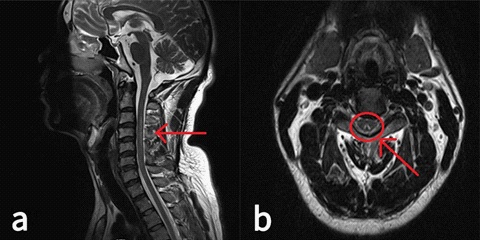
Neurological examination revealed hyporeflexia and weakened deep sensation in bilateral lower extremities. The routine tests were normal, including complete blood count, urinalysis, and blood chemistries. The concentrations of homocysteine in the blood were high (45.6 umol/L), so he took folic acid and vitamin B12 according to medical advice. We further checked markers of vascular inflammation, makers of tumor, antibody of paraneoplastic syndrome and antibody of autoimmune antibody for a definitive diagnosis, they were all normal. In addition, we did a lumbar puncture. The CSF pressure was normal, but the protein in the cerebrospinal fluid was slightly high (0.53 g/L). We reviewed his MRI results in the local hospital and noted the long segmental hyperintensity changes at the posterior column from C3 to C7 level (Figure 3), which reminded us to check the serum vitamin levels. The result of serum vitamin B12 level was normal, it was likely attribute to the supplement of vitamin B12 after his hospitalization. He continued to receive vitamin B12 (0.5 mg/d) supplements by intramuscular injection. When he discharged, he reported that his numbness was relieved than before.

Case 3
The patient was a 55-year-old woman. She had high blood pressure for almost ten years and thyroid nodules was detected during a physical examination three years ago. Her diet was varied. When we saw her in the neurology ward, she told us that she began to feel hot and bulging in her upper extremities half a year ago. Three months later, the same symptoms appeared on her both lower limbs below the knee joint, worsened after walking. Notably, by asking past medical history, we realized that she became irritable and suspicious before the onset of her physical symptoms. She used to be a very good-natured person according to her husband. Thus, she took some Chinese patent medicine for menopause, but it didn’t work.
Neurological examination revealed the reduced pain perception of both hands. There were no other obvious positive signs. The routine tests including blood routine after admission were general normal. The markers of vascular inflammation, makers of tumor, antibody of paraneoplastic syndrome, antibody of autoimmune antibody, complete analysis of immunoproteins, urine Bence-Jone protein (BJP), and the concentration of homocysteine were all in normal range. But the levels of thyroid globulin antibody (TGAb, 154.7I U/ml, ≤115), thyroid peroxidase antibody (TPO-Ab, 161.6IU/ml, <34) were high, while other indicators related to the thyroid gland were normal. NCV showed that the latent period of the motor nerve conduction of the right median nerve was prolonged, and the sensory conduction velocity of the bilateral median nerve was decreased. F-wave and H-reflex were normal. Analysis of the cerebrospinal fluid showed the number of white blood cells is 10 X 106 /L (0-8), others were normal. To find out more, we suggested a gastric endoscopy examination and MRI scan of cervical spine, but she refused.
She was treated with small dose of methylprednisolone for a few days. However, she became more agitated during the medication. Accompany with the deteriorative psychiatric symptom, we further checked the serum vitamin B12 concentration with the results of 77 pg/ml (187-883). We immediately adjusted our treatment and supplied her with a dose of Vitamin B12 0.5 mg/d and Vitamin B1 100 mg/d. At discharge, the patient felt a little bit improvement in her symptoms.
Table 1: Summary of clinical features in 9 cases of subacute combined degeneration in our hospital in recent five years.
Case |
Sex |
Age |
Initial symptoms |
Digestive system disease |
Spinal cord |
Laboratory |
|
1 |
F |
63 |
Both legs numbness and weakness |
Hyperintensity changes at the posterior and lateral column (C3-T11) |
Hb 47 g/L, |
||
2 |
M |
41 |
Both hands numbness |
- |
hyperintensity changes at the posterior column (C3-C7) |
Hb 163 g/L, |
|
3 |
F |
55 |
Personality change |
- |
- |
Hb 134 g/L, |
|
4 |
M |
81 |
Both hands numbness |
- |
hyperintensity changes at the posterior column (C3-C6) |
Hb 109 g/L, |
|
5 |
M |
68 |
Both legs |
Subtotal gastrectomy |
normal |
Hb 123g/L, |
|
6 |
M |
72 |
Both legs |
- |
- |
Hb 65 g/L, |
|
7 |
F |
66 |
Both hands |
Partial proctectomy |
hyperintensity changes at the posterior column (C3-C6) |
Hb 119 g/L, |
|
8 |
M |
64 |
Both legs |
Chronic colitis, gastric ulcer |
normal |
Hb 137 g/L, |
|
9 |
M |
73 |
Four limbs numbness, |
- |
normal |
Hb 121 g/L, |
|
Table 2: A comparison of clinical features of case 1: prior and after treatment.
|
Prior treatment |
After treatment |
Symptoms |
Four limbs numbness and weakness, ataxia, lost the ability of ambulation |
Right leg numbness |
Physical examination |
hypesthesia in four limbs, decreased proprioception in both legs,absent knee and achilles jerk |
hypesthesia in right leg |
Hb |
49 |
127 |
MCV |
117.1 |
86.3 |
Vitamin B12 |
10 |
450 |
MRI scan |
Sagittal T2-weighted imaging showed hyperintensity in the dorsal column of the cervicothoracic |
Sagittal T2-weighted and axial T2-weighted imaging showed that the abnormal signal disappeared |
Discussion
Clinically, the middle-aged group is in high-risk of SCD. According to the International Journal of Epidemiology analysis, the average age of the deficiency of vitamin B12 is at about 60 years old 2-4. There are a wide variety of the reason of lack of vitamin B12. Firstly, unhealthy diet such as vegan or excessive diet contributes to the anomalous absorption of B12. Besides, digestive system disorders such as atrophic gastritis, stomach ulcers, subtotal gastrectomy, and bowel resection are used to be the common causes of SCD. However, with the improvement of medical treatment, the cause of SCD has been deeply understood. Long term use of medications such as metformin, proton-pump inhibitor, and H2 receptor antagonist can reduce B12 intake 3, 4. A study of 799 patients who received metformin for at least 3 months showed that metformin could lead to a decrease in vitamin B12 levels, especially over a period of 4 years, with a significant decrease in the mean daily dose of > 1000 mg [5]. A related meta-analyses also suggested that taking metformin could reduce vitamin B12 levels [6].
Some scholars have also found that thyroid hormones promote the normal function of the digestive system. Excess or deficiency of thyroid hormone can lead to absorption disorders of vitamin B12 [7]. In our case 3, the levels of TGAb and TPO-Ab were beyond the normal range, while thyroid hormones were normal. Whether the antibody of thyroid could also contribute to the absorption disorders of B12 needs further research. And previous studies have shown that 40.5% of patients with hypothyroidism were also associated with vitamin B12 deficiency. Zhu Haibing et al. analyzed 17 patients with SCD and found that 35.3% of them had subclinical hypothyroidism [7,8]. But others point out that there is not enough evidence to test regular screening of vitamin B12 levels in hypothyroidism patients unless they have an autoimmune thyroid disease [9].
Genetic factors may also be responsible for SCD. According to a new report, some patients were found with a genetic defect in transcobalamin. The disease is an autosomal recessive disorder, causing decreased levels of stored vitamin B12 and functional vitamin B12. Usually, serum vitamin B12 levels are normal while levels of homocysteine are high [3]. Nitrous Oxide (N2 O) is aanesthetic and analgesic drug. Nowadays, it is often abused by young people who are blindly seeking pleasure [10]. Nitrous oxide interacts with vitamin B12 in elective inhibition of methionine synthetase and directly affects DNA synthesis and nerve axon integrity [11]. In a word, nitrous oxide induces subacute combined degeneration through the inactivation of the vitamin B12 metabolism [10,12,13]. Therefore, it reminds us that we should ask whether they have the past history of inhalation of N2 O when facing healthy young man.
The patient in our case 2 did not have a clear result of decreasing vitamin B12 level. But even if the level of vitamin B12 was within the normal range, the phenomenon could also be explained. Normal serum vitamin B12 level doesn’t mean it has a normal utility of B12 in the organization [14]. Patients with normal serum vitamin B12 may also have anormal serum transcobalamin TC, which can improve the efficiency of vitamin B12 uptake by cells through TC receptor mediated catalysis. Through enzymatic reactions, vitamin B12 binds in the mitochondria and cytoplasm to form active forms of adenosylcobalamin and mecobalamin, which act as catalysts to convert methylmalonephthalide CoA (CoA) and Hcy to succinyl CoA methionine respectively [15]. Therefore, if patients have severe vitamin B12 deficiency, they will have severe high levels of Methylmalonic Acid (MMA) and Hcy.
Hematological symptom of SCD usually appears as Megaloblastic Anemia (MA) [9]. MA is a developmental disorder of nucleus and cytoplasm caused by the deficiency of folate or vitamin B12 [16]. In all types of anemia, Mean Corpuscular Volume (MCV) and Red Cell Distribution Width (RDW) of MA is of great specificity. However, sometimes MA can represent as three series decreasing in the blood routine. Thus, MA should be distinguished from Myelodysplastic Syndrome (MDS). Both of the two diseases have obscure onset and progressive aggravation, along with obvious anemia symptoms, which are easy to be misdiagnosed. MDS is one of the malignant clonal diseases derived from hematopoietic stem cell. The disease is marked by the reduction of one or more lines of peripheral blood cells [17]. The diagnostic treatment is effective in differentiation between the two diseases. Patients of MA would have a good prognosis to a great extent with the supplement of folic acid and/or vitamin B12. If necessary, histocytochemical staining, molecular biology and flow cytometric immunophenotypic analysis can be used for comprehensive consideration.
As an objective indicator of nerve damage, neuroelectrophysiology is more reliable than subjective sensation. Some experts believe that spinal nerve conduction velocity can provide the basis for the early diagnosis of SCD [18].
MRI can identify the lesion and extent of SCD, which is not only important for early diagnosis and differential diagnosis, but also valuable for clinical follow-up. In MRI, SCD is mostly manifested as cervicothoracic posterior cord and/or lateral cord, symmetrical long T1 and long T2 signals. It is usually not enhanced and is inverted V-shaped at the axial position. The upper thoracic posterior cord is usually the first to be involved, and then expands to the upper and lower direction, gradually involving the lateral cord, and further involving the anterior cord and gray matter. White matter lesions are often heavier than gray matter [3]. The lesion reported in this paper were all located in the cervical and/or thoracic regions. In case 1, after a few months of vitamin B12 treatment, the abnormal signals in MRI were completely disappeared. A study had shown that SCD in the chronic stage was dominated by fibrous hyperplasia, and the glial cell hyperplasia was not obvious, so MRI performance could be normal [19].
Most patients with SCD have a subacute or chronic onset, and the symptoms develop gradually. Thus, there is generally no particular time of SCD onset. Meanwhile, SCD lacks of characteristic symptoms and signs. It’s known to all that the main clinical manifestations are limb paresthesia, spasmodic dyskinesia and ataxia, but the rare clinical manifestations just like mental symptoms, cognitive impairment and dysphagia are easily forgotten.
To sum up, the prognosis of SCD is time-dependent. Therefore, the clinicians should be familiar with the atypical characteristics of SCD and can combine the pre-existing conditions, clinical symptoms and correlated laboratory examinations to make quick and accurate diagnosis.
Highlights
● Three middle-aged patients didn’t got the right diagnosis in the first place. ● The causes of SCD has been deeply understood. ● SCD isn’t usually associated with a clear result of decreasing vitamin B12 level. ● MA can represent as three series decreasing in the blood routine. ● Mental symptoms, cognitive impairment and dysphagia can also be the clinical manifestations of SCD.
Declarations
Consent to publish: Not applicable.
Availability of data and materials: The data generated during the current study are available from the corresponding author on reasonable request.
Competing interests: The authors declare that they have no conflict of interest.
Funding: The present study was funded by the National Key R&D Program of China (2017YFE0103700).
Authors’contributions: Xiuying Caiand Yuan Liu designed this study. Anqi Tang and Tan Licollected and analyzed the patient data, and were the major contributor in writing the manuscript. Zhi Wang and Qianqian Ding conducted the follow-up of participants. All authors contributed to creating this manuscript and improved the final version.
Acknowledgments: We thank the Department of Neurology and Radiology of The First Affiliated Hospital of Soochow University (Suzhou, China) for their helpful and continuous support.
References
- Wang YH, Yan F, Zhang WB, Ye G, Zheng YY, Zhang XH, et al. An investigation of vitamin B12 deficiency in elderly inpatients in neurology department. Neurosci Bull. 2009; 25: 209-215.
- Healton EB, Savage DG, Brust JC, Garrett TJ, Lindenbaum J, et al. Neurologic aspects of cobalamin deficiency. Medicine (Baltimore) 1991; 70: 229-245.
- Jain KK, Malhotra HS, Garg RK, Gupta PK, Roy B, et al. Prevalence of MR imaging abnormalities in vitamin B12 deficiency patients presenting with clinical features of subacute combined degeneration of the spinal cord. J Neurol Sci. 2014; 342: 162-166.
- Matsuura H, Nakamura T. Inverted V sign: Subacute combined degeneration of the spinal cord. QJM. 2018; 111: 65-66.
- Chapman LE, Darling AL, Brown JE. Association between metformin and vitamin B12 deficiency in patients with type 2 diabetes: A systematic review and meta-analysis. Diabetes Metab. 2016; 42: 316-327.
- Hasan NU, Makki MU, Abid I, Abid Butt MUR. Association of Vitamin B12 Deficiency with Intake of Oral Metformin in Diabetic Patients. J Ayub Med Coll Abbottabad. 2019; 31: 72-75.
- Sun G, Shi YB. Thyroid hormone regulation of adult intestinal stem cell development: Mechanisms and evolutionary conservations. Int J Biol Sci. 2012; 8: 1217-1224.
- Jabbar A, Yawar A, Waseem S, Islam N, Ul Haque N, Zuberi L, et al. Vitamin B12 deficiency common in primary hypothyroidism. J Pak Med Assoc. 2008; 58: 258-261.
- Collins AB, Pawlak R. Prevalence of vitamin B12 deficiency among patients with thyroid dysfunction. Asia Pac J Clin Nutr. 2016; 25: 221-226.
- Garakani A, Jaffe RJ, Savla D, Welch AK, Protin CA, et al. Neurologic, psychiatric, and other medical manifestations of nitrous oxide abuse: A systematic review of the case literature. Am J Addict 2016; 25: 358-369.
- Stacy CB, Di Rocco A, Gould RJ. Methionine in the treatment of nitrous-oxide-induced neuropathy and myeloneuropathy. J Neurol. 1992; 239: 401-403.
- Sanders RD, Weimann J, Maze M. Biologic effects of nitrous oxide: A mechanistic and toxicologic review. Anesthesiology. 2008; 109: 707-722.
- Stockton L, Simonsen C, Seago S. Nitrous oxide-induced vitamin B12 deficiency. Proc (Bayl Univ Med Cent). 2017; 30: 171-172.
- Roessler FC, Wolff S. Rapid healing of a patient with dramatic subacute combined degeneration of spinal cord: A case report. BMC Res Notes. 2017; 10: 18.
- Jongen JC, Koehler PJ, Franke CL. [Subacute combined degeneration of the spinal cord: Easy diagnosis, effective treatment]. Ned Tijdschr Geneeskd. 2001; 145: 1229-1233.
- Socha DS, DeSouza SI, Flagg A, Sekeres M, Rogers HJ. Severe megaloblastic anemia: Vitamin deficiency and other causes. Cleve Clin J Med. 2020; 87: 153-164.
- Falco P, Levis A, Stacchini A, Ciriello MM, Geuna M, Prognostic relevance of cytometric quantitative assessment in patients with myelodysplastic syndromes. Eur J Haematol. 2011; 87: 409- 418.
- Hemmer B, Glocker FX, Schumacher M, Deuschl G, Lucking CH, et al. Subacute combined degeneration: Clinical, electrophysiological, and magnetic resonance imaging findings. J Neurol Neurosurg Psychiatry. 1998; 65: 822-827.
- Murata S, Naritomi H, Sawada T. MRI in subacute combined degeneration. Neuroradiology. 1994; 36: 408-409.