
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Spiderweb omentum – A previously unknown surgical finding in ovarian cancer
Mukurdipi Ray*; Madiwalesh Chhebbi
All India Institute of Medical Sciences, New Delhi, India
*Corresponding Author: Mukurdipi Ray
Additional Professor, Department of Surgical Oncology, All India Institute of Medical Sciences, New
Delhi, India.
Email: drmajormdrayaiimsdelhi@aiims.edu
Received : Feb 09, 2022
Accepted : Mar 14, 2022
Published : Mar 21, 2022
Archived : www.jcimcr.org
Copyright : © Ray MD (2022).
Abstract
Carcinoma ovary is the most lethal gynecological malignancy and thereby, leading cause of death worldwide. Most common histopathology of ovarian cancer is high-grade serous carcinoma. More than 75% patients present at advanced stages, FIGO stage III onwards. The response of chemotherapy in patients is variable and the surgical finding of the state of omentum following chemotherapy has not been described specifically in literature. Here we presented a case of carcinoma ovary whose omental caking totally dissolved after chemotherapy leaving behind only the vasculature resembling a spiderweb. Though the treatment policy was the same.
Keywords: Carcinoma ovary; Neoadjuvant Chemotherapy; Omental caking; Spiderweb omentum.
Citation: Ray M D, Chhebbi M. Spiderweb omentum – A previously unknown surgical finding in ovarian cancer. J Clin Images Med Case Rep. 2022; 3(3): 1749.
Introduction
Carcinoma ovary is the most lethal gynecological malignancy and thereby, leading cause of death worldwide. According to GLOBOCAN 2020 estimates, ovarian malignancies accounted for 1.6% of newly diagnosed malignancies and resulted in 2.1% of all malignancy-related reported deaths [1].
Most common histopathology of ovarian cancer is highgrade serous carcinoma. More than 75% patients present at advanced stages, FIGO stage III onwards. Epithelial ovarian cancer has a predilection for the omentum as the site of metastasis. The involvement of omentum is classified under FIGO grading stage IIIB which includes macroscopic peritoneal metastases less than 2 cm and IIIC with more than 2 cm metastases [2].
Omentectomy has now become a standard part of cytoreductive surgery being carried out for ovarian cancers, even in the absence of tumor deposits in the omentum. Iwagoi et al note that patients with poor response to chemotherapy for omental metastasis had poor survival as compared to those patients with good response in advanced ovarian cancers [3].
The standard treatment option for Carcinoma Ovary is upfront cytoreductive surgery (CRS) followed by systemic chemotherapy. Neoadjuvant Chemotherapy followed by interval CRS is the option when primary CRS is not amenable due to poor performence status or others various factors [4].
The response of chemotherapy in patients is variable and the surgical finding of the state of omentum following chemotherapy has not been described specifically in literature. Here we present a case of a patient with carcinoma ovary whose omental caking responded very well to chemotherapy leaving behind only the vasculature resembling a spiderweb.
Case report
A 60-year-old lady presented with a history of abdominal pain of three months duration to our OPD in our tertiary care referral oncology center. On initial imaging findings done via PET CT showed ascites, pelvic masses, omental and peritoneal deposits along with omental caking in the form of thickness with enhancement similar to other peritoneal deposits and ovarian masses. Her biopsy from omental deposits showed features of serous carcinoma ovary with cells being diffusely and strongly positive for WT-1 and p53. She was diagnosed with serous carcinoma ovary, stage IIIC as per CT PCI and Because of her poor performance status, she underwent neoadjuvant chemotherapy and was given 9 cycles of weekly chemotherapy of paclitaxel and carboplatin and was taken up for interval cytoreductive surgery.
Post chemotherapy on clinical examination a 25 X 20 cm, hard abdominopelvic mass involving the lower quadrants of the abdomen. Prior to her surgery, a contrast-enhanced computed tomography showed partial response. In this case, the omental caking had been reported to have reduced and only haziness in the omentum was reported.
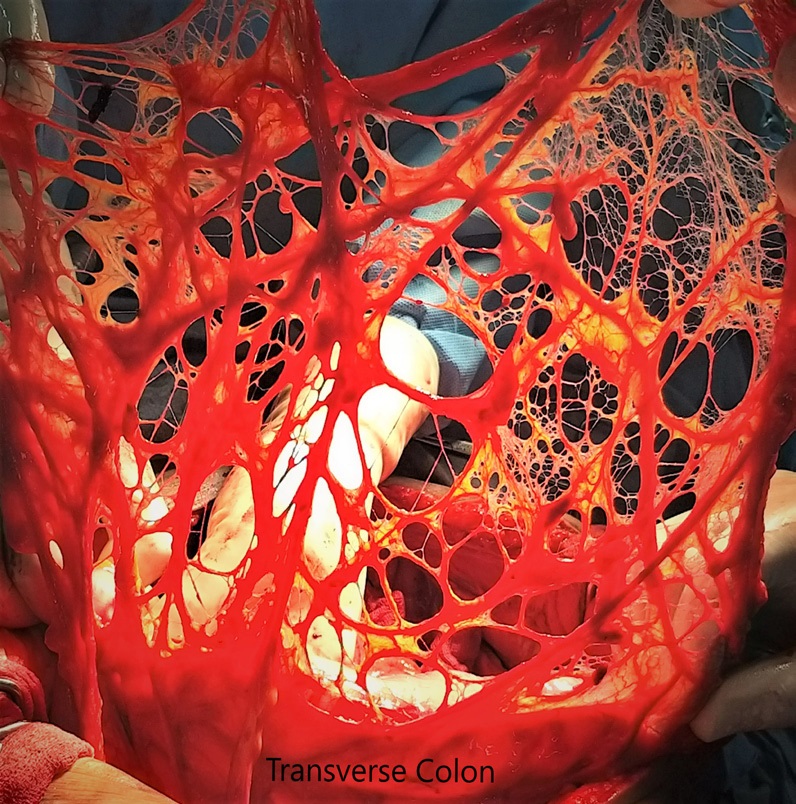
On exploratory laparotomy, it was found that omentum is totally fat and toumor less i.e., omental caking dissolved completely; leaving behind the vascular structures only. Surprisingly the vascular framework resembling a spiderweb (Figure 1). Other operative findings included a large solid cystic right adnexal mass approximately 12 X 10 cm and a smaller 6 X 6 cm left adnexal mass. Multiple peritoneal deposits were noted in subdiaphragmatic region and on liver surface. She also had enlarged external iliac nodes. The patient underwent optimal cytoreduction surgery (CRS) including total omentectomy followed by hyperthermic intraperitoneal chemotherapy and had an uneventful post-operative period. The final histopathology revealed bilateral adnexal high grade serous carcinomas with capsular breach along with several peritoneal deposits. The omentum showed a chemotherapy response score of 2.
Discussion
The omentum is a large fold of the peritoneum which hangs down from the greater curvature of the stomach and covers the loops of intestines to a variable extent and is made up of four layers fused together and contain variable amounts of fat along with small arteries and veins. The lesser omentum is another fold of the peritoneum extending from the lesser curvature of the stomach and the first part of the duodenum to inferior surface the liver. Microscopically the omentum consists of thin fenestrated translucent membranes and adipose-rich areas [5]. Intraperitoneal spread of ovarian malignancies has been known to occur in the peritoneum of the pelvis, lesser and greater omentum, paracolic gutters, livers Glisson diaphragm, and diaphragmatic peritoneum. Soft tissue thickening, nodularity, and all are the signs of peritoneal involvement [6]. The tumor cells traverse the peritoneum through the “transcoelomic” spread with the omentum being the most common site of these metastases [7].
Böhm et al. developed a Chemotherapy Response Score (CRS) - a three-tier grading system in 2015 following omental assessment of residual disease after neoadjuvant chemotherapy in a cohort of 71 epithelial ovarian carcinoma patients. The scoring system can be described as follows:
Score 1: No or minimal tumor response (mainly viable tumor with no or minimal regression-associated fibro-inflammatory changes, limited to a few foci);
Score 2: Partial tumor response (multifocal or diffuse regression, with viable tumor ranging from diffuse sheets, streaks, or nodules, to extensive regression with multifocal but easily identifiable residual tumor);
Score 3: Complete or near-complete response (few irregularly scattered individual tumor cells or cell groups, all measuring <2 mm, or no residual tumor identified) [8].
In ovarian carcinoma, several prognostic factors have been described to date. The omental residual disease is now emerging as a significant prognostic factor with CRS showing a significant prognostic value for both overall survival and progressionfree survival [4,8].
Radiological response assessment in the form of Peritoneal Cancer Index (PCI) has been evaluated by several authors and is considered as a reliable method in the assessment of disease and evaluation of incomplete cytoreduction in advanced epithelial ovarian cancers. Patients with higher PCI on radiology could be subjected to chemotherapy But NACT should not be the alternative to poor surgical skill [9,10].
Surgical PCI is the macroscopic assessment of tumor by the surgeon as an intraoperative finding and its value ranges from 0-39. Studies suggest that PCI represents a better correlation of extent of disease and prognostic information [11].
Conclusion
In ovarian cancer omentectomy is the integral part of CRS. Typical description of omentum losing all its adipose tissue and tumor ie caking in response to chemotherapy, has not been described previously making this pictorial description of ‘spiderweb omentum’ an interesting and rare finding. But the surgical principle would be the same
Conflicts of interest: None
Financial support: None
References
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021; 71: 209–249.
- Prat J, Committee F. International Journal of Gynecology and Obstetrics Staging classification for cancer of the ovary , fallopian tube , and peritoneum. Int J Gynecol Obstet [Internet]. 2014; 124: 1–5. Available from: http://dx.doi.org/10.1016/j. ijgo.2013.10.001
- Iwagoi Y, Motohara T, Hwang S, Fujimoto K, Ikeda T, Katabuchi H, et al. Omental metastasis as a predictive risk factor for unfavorable prognosis in patients with stage III–IV epithelial ovarian cancer. Int J Clin Oncol [Internet]. 2021; 26: 995–1004. Available from: https://doi.org/10.1007/s10147-021-01866-3
- M D Ray et al. Upfront Cytoreductive Surgery versus Neoadjuvant Chemotherapy in advanced Epithelial Ovarian Cancer in Indian patients. 10.2217/fon-2021-0077
- Collins D, Hogan AM, O’Shea D, Winter DC. The omentum: Anatomical, metabolic, and surgical aspects. J Gastrointest Surg. 2009; 13: 1138–1146.
- Nougaret S, Addley HC, Colombo PE, Fujii S, Al Sharif SS, Tirumani SH, et al. Ovarian carcinomatosis: How the radiologist can help plan the surgical approach. Radiographics. 2012; 32: 1775– 1800.
- Ma X. The omentum, a niche for premetastatic ovarian cancer. J Exp Med. 2020; 217: 4–6.
- Böhm S, Faruqi A, Said I, Lockley M, Brockbank E, et al. Chemotherapy response score: Development and validation of a system to quantify histopathologic response to neoadjuvant chemotherapy in tubo-ovarian high-grade serous carcinoma. J Clin Oncol. 2015; 33: 2457–2463.
- Jónsdóttir B, Lomnytska M, Poromaa IS, Silins I, Stålberg K. The Peritoneal Cancer Index is a Strong Predictor of Incomplete Cytoreductive Surgery in Ovarian Cancer. Ann Surg Oncol. 2021; 28: 244–251.
- Elzarkaa AA, Shaalan W, Elemam D, Mansour H, Melis M, et al. Peritoneal cancer index as a predictor of survival in advanced stage serous epithelial ovarian cancer: A prospective study. J Gynecol Oncol. 2018; 29: 1–10.
- Elzarkaa AA, Shaalan W, Elemam D, Mansour H, Melis M, et al. Peritoneal cancer index as a predictor of survival in advanced stage serous epithelial ovarian cancer: A prospective study. J Gynecol Oncol. 2018; 29: 1–10.