
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
Intestinal perforation after extracorporeal lithotripsy; Possibility of nonoperative management
Pablo Fernández Galeano*; Cristina Rodriguez Silva; María del Pilar Gutiérrez Delgado; Rosa Perez Rodriguez; Julio Santoyo
Regional University Hospital of Malaga, Malaga, Spain.
*Corresponding Author: Pablo Fernandez Galeano
Regional University Hospital of Malaga, Malaga, Spain.
Email: fernandezg_7@hotmail.com
Received : Feb 09, 2022
Accepted : Mar 15, 2022
Published : Mar 22, 2022
Archived : www.jcimcr.org
Copyright : © Galeano PF (2022).
Citation: Galeano PF, Silva CR, Delgado MPG, Rodriguez RP, Santoyo J. Intestinal perforation after extracorporeal lithotripsy; Possibility of Nonoperative management. J Clin Images Med Case Rep. 2022; 3(3): 1750.
Introduction
Extracorporeal Shock wave Lithotripsy (ESWL) has proved to be effective safe and nowadays is the preferred method of treatment of over 90% of upper urinary tract stones [1,2]. Nevertheless, ESWL is not devoid of complications. Although the majorities are trivial and transient, serious complications could occur but are extremely rare and only very few have been reported in the literature [3].
We report a case of small intestinal perforation following ESWL. The case is striking because we decided to carry out a non-operative management, which in this case turned out to be successful. We are not aware of another such case in the English-language literature.
Case report
A 56-year-old woman with a history of recurrent reno-ureteral colic requiring several sessions of Extracorporeal Lithotripsy (ESWL). She was admitted to the emergency department of our center due to abdominal pain focused on the left hemiabdomen after the last ESWL session 48 hours ago, associated with nausea, vomiting and haematuria.
On physical examination, she presented pain in the left hemiabdomen without signs of peritoneal irritation.
Laboratory tests showed elevated Leukocytes (19010/µl, Neutrophilia 92% and CRP 279 mg/L).
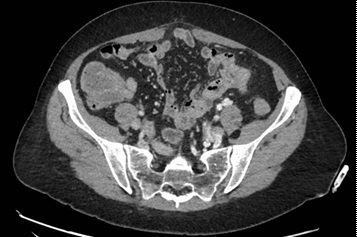
CT was performed showing inflammatory changes and gas in the wall of a segment of the small bowel, located adjacent to treated ureteral lithiasis, compatible with perforation of the small intestine secondary to ESWL (Figure 1).

The patient was hemodynamically stable and the pain was not increasing.
We decided to carry out a non-operative management, with antibiotic therapy and digestive control, evolving favorably.
Control CT was performed 7 days later with evident radiological improvement (Figure 2).
Discussion
ESWL is widely used as a safe and effective technique. Complications involving the gastrointestinal tract are rare, however they can be potentially very serious.
It is described that the use of high energy or the prone position can behave as risk factors. Reviewing the literature, we have found few cases of intestinal perforation after an ESWL session. In all of them, the presence of peritoneal irritation or hemodynamic instability made necessary an urgent surgical intervention. In this case, the clinical situation allowed us to carry out a non-operative management, as we would have done with the same clinical picture with a different etiology. We therefore consider that in the absence of signs of peritonitis and hemodynamic instability, selected cases of bowel perforation after ESWL can be safely treated conservatively.
References
- Chaussy C, Schmiedt E, Jocham D et al. First clinical experience with extracorporeally induced destruction of kidney stones by shockwaves. J Urol. 1982; 127: 417.
- Streem SB. Contemporary clinical practice of shock wave lithotripsy: Re-evaluation of contraindications. J Urol. 1997; 157: 1197-1203.
- Fuchs GJ, David RD, Fuchs AM. Complications of extracorporeal shockwave lithotripsy. Arch Esp Urol. 1989; 42: 83-89.