
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Correlation analysis of TCM syndrome characteristics and high risk factors of patients with colorectal polyps in Shenzhen: A case retrospective study
Ying Sun; Chao Huang*
Department of Traditional Chinese Medicine, The Second Affiliated Hospital of Shenzhen University (People’s Hospital of Shenzhen Baoan District), Shenzhen 518100, China.
*Corresponding Author: Chao Huang
Department of Traditional Chinese Medicine, The
Second Affiliated Hospital of Shenzhen University,
Shenzhen 518100, China.
Email: huangchao06@163.com
Received : Feb 09, 2022
Accepted : Mar 16, 2022
Published : Mar 23, 2022
Archived : www.jcimcr.org
Copyright : © Huang C (2022).
Abstract
Objective: To analyze the characteristics of Traditional Chinese Medicine (TCM) asthenia- and sthenia-syndrome and its correlation with high-risk factors in patients with colorectal polyps in Shenzhen through case retrospective study
Methods: 296 eligible patients hospitalized were collected in the Department of TCM in People’s Hospital of Shenzhen Baoan District from January 2016 to June 2021, and diagnosed with intestinal polyps, and divided into deficiency-syndrome, sthenia-syndrome and Asthenia-Syndrome Accompanied With Sthenia-Syndrome (ASASS). In addition, the correlation between syndromes and hyperglycemia, hypertension, hyperlipidemia and hyperuricemia was also analyzed.
Results: There were 37 patients with ASASS, among which deficiency of vital energy and blood stasis accounted for the highest proportion. For patients with ASASS, the age difference among different syndromes was statistically significant (P<0.05). The proportion of patients with hypertension and sthenia of liver yang was significantly higher than that of other syndromes (P<0.05).
Conclusion: Patients with colorectal polyps in Shenzhen area are mainly deficiency of vital energy and phlegm-wetness, and the pathological factors involve phlegm-dampness, blood stasis and stagnation of vital energy. Age and hypertension should be considered in the treatment of ASASS.
Keywords: colorectal polyps; TCM syndrome; asthenia-syndrome accompanied with sthenia-syndrome; deficiency of vital energy; Shenzhen.
Citation: Sun Y, Huang C. Correlation analysis of TCM syndrome characteristics and high risk factors of patients with colorectal polyps in Shenzhen: A case retrospective study. J Clin Images Med Case Rep. 2022; 3(3): 1753.
Introduction
In January 2021, a paper was published in the internationally famous journal (J Nat Cancer Center) and pointed out that the incidence of colorectal cancer in domestic population increased significantly in China from 2000 to 2015 after age standardization, especially in urban areas [1], which may be due to the general application of endoscopic screening and early removal of various polyps.
Although most colorectal polyps are benign tumors, most colorectal cancers are evolved from polyps or adenomas, namely, polyp-adenoma-cancer pathway [2,3], so it is of great clinical significance for early detection, diagnosis and treatment of colorectal polyps. As we all know, tumors in gastrointestinal system are closely related to living habits [4-6]. These bad habits include alcoholism, deep-frying, barbecue, high-salt and high-fat diet, coupled with environmental changes and fast life rhythm, such as staying up late, high-load work and other factors, which damage the body’s immune defense function and lead to the occurrence of benign and malignant tumors including polyps [7]. These factors comprehensively act on the human, resulting in different physical changes. In traditional Chinese medicine, it is considered that these factors may be one of the factors causing different syndromes.
Shenzhen is located in Guangdong province, China, belongs to Lingnan area, and its climate is warm, rainy and humid. This unique climate can form unique physiological and pathological characteristics [8]. However, so far there are no relevant researches on the distribution of TCM syndromes and related risk factors of patients with colorectal polyps in Shenzhen. Therefore, this paper discussed the distribution of TCM syndromes in patients with colorectal polyps in Shenzhen, and analyzed the correlation between related risk factors and TCM syndromes.
Methods
Case data
This was a case retrospective study design. The patients who underwent electronic colonoscopy in the Department of Traditional Chinese Medicine (People’s Hospital of Shenzhen Baoan District) were collected according to the inclusion and exclusion criteria from January 2016 to June 2021. The basic information including registration number, age, sex, admission diagnosis and TCM syndromes were recorded. A total of 296 eligible patients aged 27-83 (52.62 ± 9.85) were researched in this study, including 174 male patients (58.8%) and 122 female patients (41.2%).
Diagnostic criteria
Diagnostic criteria of TCM: TCM syndrome types refer to “Diagnostic Criteria for Common TCM Syndrome” [9], and “Internal Medicine of Traditional Chinese Medicine” published by Zhou Zhongying [10]. The syndromes are jointly determined by an attending physician and a senior doctor
Diagnostic criteria of western medicine: Colon polyps or rectal polyps were diagnosed according to electronic colonoscopy.
Inclusion criteria
These patients had no household registration and lived in Shenzhen for more than 5 years, and conformed to the diagnostic criteria of colorectal polyps. The age was over 18 years old. All patients had been examined by electronic colonoscopy.
Exclusion criteria
These patients had a history of colonic polyps in the past but could not provide a detailed examination report or did not find polyps after colonoscopy again. Patients had incomplete case data or familial adenomatous polyposis or colon cancer confirmed by pathological diagnosis.
Complicating diseases
We also collected the complicating diseases, that is, whether there was hyperglycemia, hypertension, hyperlipidemia and hyperuricemia (4H). The diagnostic criteria of the diseases were as follows: hyperglycemia (fasting blood glucose >6.1 mmol/L), hypertension (systolic blood pressure >140 mmHg or diastolic blood pressure >90 mmHg), hyperlipidemia (total cholesterol >5.17 mmol/L or triglyceride >1.43 mmol/L)
Statistical analysis
All the data in this study were performed by SPSS 23.0. The measurement data was presented by mean and standard deviation. One-Way ANOVA was used for comparison of age among multiple groups, and LSD method was used for multiple comparison among groups, The correlation of age with TCM syndromes was analyzed by Pearson Correlation Coefficient. The qualitative data including sex and complicating diseases were presented by proportion, and the overall distribution among groups was analyzed by Chi-square test, and the correlation was evaluated by Spearman Coefficient. P<0.05 was considered to be that the difference was statistically significant.
Result
Basic information of patients with various TCM syndromes
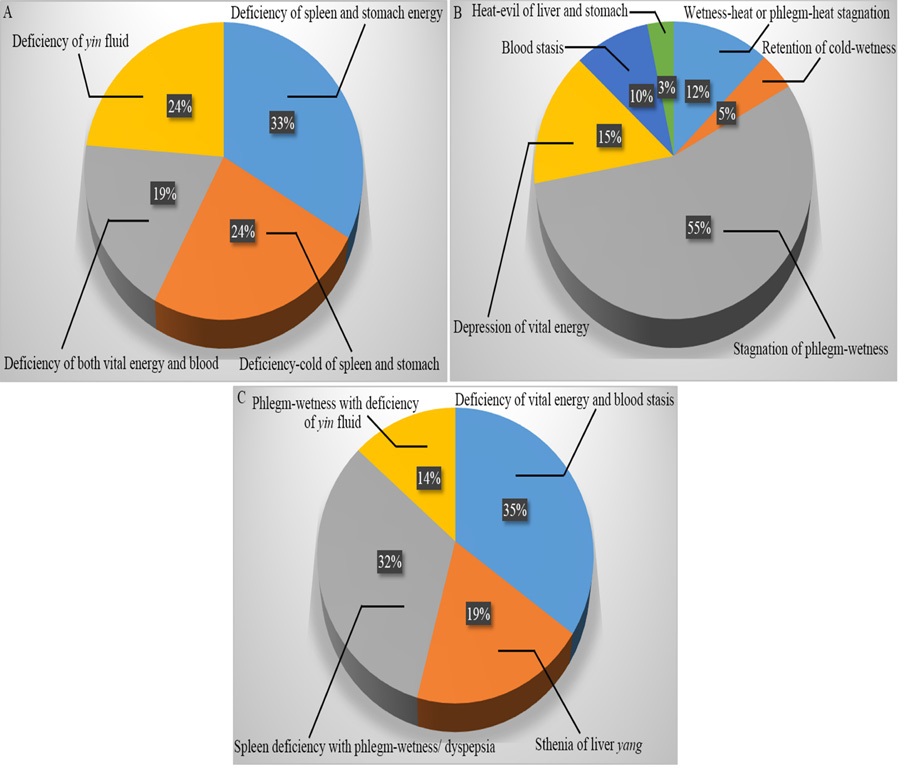
A total of 296 eligible patients with colorectal polyps were collected in this study. 80 patients were deficiency-syndrome, and the highest proportion of patients (33%) was deficiency of spleen and stomach energy, followed by deficiency-cold of spleen and stomach (cold-syndrome due to deficiency of spleen and stomach-yang) and deficiency of yin fluid, each accounting for 24% (Figure 1A). There were 179 patients with sthenia-syndrome, among which the highest proportion was the stagnation of phlegm-wetness (55%), followed by stagnation of vital energy and damp-heat or phlegm-heat, which were 15% and 12% respectively (Figure 1B). Among them, damp-heat/phlegm-heat was mainly wetness-heat in large intestine or phlegm-heat stagnation in lung. There were 37 patients with Asthenia-Syndrome Accompanied With Sthenia-Syndrome (ASASS), of which the highest proportion was deficiency of vital energy and blood stasis, accounting for 35%, followed by deficiency of spleen energy and phlegm dampness/dyspepsia syndrome, accounting for 32% (Figure 1C).
Appearance of intestinal polyps of all patients under electronic colonoscope
As shown in Figure 2, appearance of intestinal polyps of all patients under electronic colonoscope was different. The polyps in the patients with asthenia-syndrome were light, pale and tender, especially in the these with deficiency of spleen and stomach energy, deficiency-cold of spleen and stomach, and deficiency of both vital energy and blood. While the intestinal mucosa was thin and the blood vessels were obviously exposed (Figure 2A). On the contrary, significant hyperemia and edema was be found in the colon mucosa of the patients with stheniasyndrome (Figure 2B), especially in the patients with wetnessheat or phlegm-heat stagnation, and heat-evil of liver and stomach. The blood vessels in the mucosa was purple and visible in the patients with blood stasis. As for the patients with ASASS, the mucosa was obviously marked with edema, while the polyps in the colon with phlegm-wetness with deficiency of yin fluid was red and swollen, and the blood vessels were clearly visible (Figure 2C).
Comparison of age and sex distribution of all patients
The results revealed that there were more men (47 cases) than women (33 cases) in the deficiency-syndrome group (Table 1), but there is no statistical difference in the overall distribution of gender among various deficiency syndromes, and there is no statistical difference in the average age between each group. As shown in Table 2, there were 102 male patients in the stheniasyndrome group, which was higher than 77 female patients, but there is no significant difference in the overall distribution among the groups. Although the age of patients with wetnessheat and phlegm-heat stagnation was lower than that of patients with other syndromes, there was no significant difference in the mean value among the groups. Similarly, there were more male patients than female patients in ASASS group (P>0.05), however, there was a significant difference in age between each group (P<0.05), and had certain correlation (Pearson coefficient was -0.451, P=0.005). As shown in Table 3, the patients with deficiency of spleen energy and phlegm-dampness/dyspepsia syndrome are the youngest, and significantly lower than those with deficiency of vital energy and blood stasis (P<0.05) and sthenia of liver yang (P<0.05).
Comparison of complicating diseases in patients with deficiency- and sthenia-syndrome
In this study, we found that some patients suffered from hyperglycemia, hypertension, hyperlipidemia and hyperuricemia (4H), so whether these “4H” diseases were related to various TCM syndromes. As shown in Table 4, there were 11 cases with hyperglycemia (14.1%), 15 cases with hypertension (19.23%), 36 cases with hyperlipidemia (46.15%) and 27 cases with hyperuricemia (34.61%) in the deficiency syndrome group. The proportion of hyperuricemia patients with deficiency of vital energy syndrome and yin deficiency syndrome was higher than that of yang deficiency syndrome and deficiency of both vital energy and blood, but the difference was not statistically significant. As shown in Table 5, the patients in the sthenia-syndrome group also suffered from “4H” diseases. There were 20 cases with hyperglycemia (11.17%), 33 cases with hypertension (18.44%), 107 cases with hyperlipidemia (59.78%), and 56 cases of hyperuricemia (31.28%). We obseved that patients with hyperlipidemia accounted for the highest proportion, but these diseases There was no significant difference between the groups. As shown in Table 6, there were 4 cases of hyperglycemia (10.81%), 11 cases of hypertension (29.73%), 21 cases of hyperlipidemia (56.76%), and 10 cases of hyperuricemia (27.03%) in patients with ASASS group. Hyperlipidemia patients accounted for the highest proportion, but there was no significant difference among the groups. The proportion of hypertension patients with sthenia of liver yang was higher than that of other syndromes (P<0.05), but there is little correlation between hypertension and ASASS syndromes (Spearman correlation coefficient was 0.078, P > 0.05).
Table 1: Comparison of age and sex distribution in deficiency syndrome groups
Groups (80 cases) |
Gender (male/female) |
Age (years) |
Deficiency of spleen and stomach energy(27 cases) |
18/9 |
55.0±9.71 |
Deficiency-cold of spleen and stomach (19 cases) |
11/8 |
51.84±9.92 |
Deficiency of both vital energy and blood (15 cases) |
6/9 |
55.6±7.32 |
Deficiency of yin fluid (19 cases) |
12/7 |
56.42±9.21 |
P value |
0.387 |
0.455 |
Table 2: Comparison of age and sex distribution in sthenia-syndrome groups
Groups (179 cases) |
Gender (male/female) |
Age (years) |
Wetness-heat or phlegm-heat stagnation(22 cases) |
16/6 |
47.86±10.26 |
Retention of cold-wetness (8 cases) |
2/6 |
53.75±13.04 |
Stagnation of phlegm-wetness (99 cases) |
58/41 |
52.75±8.81 |
Depression of vital energy (27 cases) |
15/12 |
49.30±9.95 |
Blood stasis (17 cases) |
7/10 |
55.59±10.23 |
Heat-evil of liver and stomach (6 cases) |
4/2 |
49.67±13.19 |
P value |
0.177 |
0.094 |
Table 3: Comparison of age and sex distribution in ASASS groups
Groups (37 cases) |
Gender (male/female) |
Age (years) |
Deficiency of vital energy and blood stasis (13 cases) |
10/3 |
57.0±8.89a |
Sthenia of liver yang (7cases) |
6/1 |
57.71±8.38a |
Spleen deficiency with phlegm-wetness/ dyspepsia (12 cases) |
7/5 |
44.58±11.06 |
Phlegm-wetness with deficiency of yin fluid (5 cases) |
2/3 |
48.0±8.22 |
P value |
0.287 |
0.007 |
Note: ASASS is asthenia-syndrome accompanied with sthenia-syndrome; * indicated vs spleen deficiency with phlegm-wetness/dyspepsia syndrome group P<0.05.
Table 4: Distribution and comparison results of “4H” diseases in patients with deficiency syndrome
Groups (80 cases) |
Hyperglycemia (N/Y) |
Hypertension (N/Y) |
Hyperlipidemia (N/Y) |
Hyperuricemia (N/Y) |
Deficiency of spleen and stomach energy(27 cases) |
22/5 |
20/7 |
14/13 |
17/10 |
Deficiency-cold of spleen and stomach (19 cases) |
19/0 |
17/2 |
11/8 |
17/2 |
Deficiency of both vital energy and blood (15 cases) |
13/2 |
13/2 |
8/7 |
10/5 |
Deficiency of yin fluid (19 cases) |
15/4 |
15/4 |
11/8 |
9/10 |
P value |
0.221 |
0.550 |
0.969 |
0.052 |
Note: “4H”represented Hyperglycemia, Hypertension,Hyperlipidemia, and Hyperuricemia. “N” represented no “4H”, and “Y” mean existence of “4H”(The same below).
Table 5: Distribution and comparison results of “4H” diseases in patients with sthenia-syndrome groups
Groups (179 cases) |
Hyperglycemia (N/Y) |
Hypertension (N/Y) |
Hyperlipidemia (N/Y) |
Hyperuricemia (N/Y) |
Wetness-heat or phlegm-heat stagnation(22 cases) |
18/4 |
17/5 |
10/22 |
17/5 |
Retention of cold-wetness (8 cases) |
8/0 |
7/1 |
6/2 |
7/1 |
Stagnation of phlegm-wetness (99 cases) |
88/11 |
76/23 |
43/56 |
66/33 |
Depression of vital energy (27 cases) |
26/1 |
25/2 |
14/13 |
21/6 |
Blood stasis (17 cases) |
14/3 |
15/2 |
7/10 |
8/9 |
Heat-evil of liver and stomach (6 cases) |
5/1 |
6/0 |
2/4 |
4/2 |
P value |
0.478 |
0.305 |
0.565 |
0.220 |
Table 6: Distribution and comparison results of “4H” diseases in patients with ASASS groups
Deficiency of vital energy and blood stasis (13 cases) |
Hyperglycemia (N/Y) |
Hypertension (N/Y) |
Hyperlipidemia (N/Y) |
Hyperuricemia (N/Y) |
Deficiency of vital energy and blood stasis (13 cases) |
12/1 |
11/2 |
7/6 |
8/5 |
Sthenia of liver yang (7cases) |
7/0 |
1/6 |
2/5 |
5/2 |
Spleen deficiency with phlegm-wetness/ dyspepsia (12 cases) |
9/3 |
9/3 |
4/8 |
10/2 |
Phlegm-wetness with deficiency of yin fluid (5 cases) |
5/0 |
5/0 |
3/2 |
4/1 |
P value |
0.252 |
0.003 |
0.520 |
0.648 |
Discussion
According to the results of epidemiological investigation, colorectal polyps are a very common disease in clinic [11]. Most patients have no clinical manifestations, only found during physical examination or treatment of other diseases. Although most of colorectal polyps are benign lesions, some polyps also have canceration tendency [12]. Therefore, early resection and identification of colorectal polyps are of great significance.
Although there is no name for colorectal polyps in Chinese medicine, as early as in ancient China, there are records and descriptions about the etiology and pathogenesis of polyps. For example, primitive theories documented by “The Yellow Emperor’s Canon of Internal Medicine (722-221 B.C) (Huangdi neijinig)” point out that the occurrence of polyps was related to invasion of exogenous evils. Stagnation of cold-wetness evil (a pathogenic factor blended by evils of cold and wetness) results in obstruction in the channels and stasis of vital energy and blood, leading to occurrence of polyps. (Huangdi neijinig) said, “healthy energy (referring to the resistance of the human body against diseases) existed inside, but evils could not be done”, suggesting that deficiency of healthy energy is also an important factor in the occurrence of colorectal polyps in addition to exogenous evils.
Guangdong in China belongs to the Ling’nan region. Some statistics studies on TCM syndromes of patients with colorectal polyps in Guangdong have performed, and found that deficiency of spleen-energy and evil wetness accounted for the highest proportion, followed by asthenia of the spleen and stomach and wetness-heat and blood stasis [8]. These researchers considered that deficiency of spleen-energy is the root of trouble and phlegm-evil and blood stasis are the causes of the disease. Our study found that the proportion of patients with asthenia of the spleen and stomach was the highest in all colorectal polyps patients with asthenia-syndrome in Shenzhen, which is consistent with other research results [13,14]. Our observation revealed that the proportion of patients with phlegm-evil was the highest, up to 55%, followed by stagnation of vital energy and phlegm-wetness or wetness-heat evil. Shenzhen is a southern city in Guangdong Province, and located in Ling’nan region which has a unique climate with heavy humidity and heat. These results have suggested that, tangible sthenia-evils including phlegm-wetness and blood stasis can be produced in the human body living in Shenzhen. These tangible evils can block the functional activities of vital energy for a long time, leading to depression of vital energy and further heat-syndrome resulting from disorder of vital energy. In this case, phlegm-heat or wetness-heat evil is formed, further stagnating the functional activities of vital energy in turn. Depressed vital energy, phlegm-evil and blood stasis in conflict with each other within gut and leads to occurrence of polyps. Therefore, deficiency of spleen-energy, phlegm-wetness, blood stasis and depression of vital energy are the important pathological factors of colorectal polyps [15,16]. Our study found that, in the patients with stagnation of wetness-heat, some patients suffered from stagnation of phlegmheat in the lung, which may be due to the fact that the lung and large intestine share s paired relationship, phlegm-heat evil in the lung can enter the large intestine along the channel system and block the functional activities of vital energy in gut, further affecting the blood circulation. This consequence leads to the stagnation of phlegm, depressed vital energy and blood stasis in the local intestine, resulting in formation of polyps.
It is considered that the occurrence of colorectal polyps is the results of many risk factors. Although these factors are related to histological type of polyps and family history [17], other risks have been paid more and more attention. Some studies have shown that age is considered as one of the risk factors related to the occurrence of colorectal polyps [18-20]. The older the age, the higher the incidence of colorectal polyps, especially after 40 years old [21]. This is consistent with the observation of our study. We found that the average age of polyp patients is over 50 years old. This may be related to the decrease of intestinal peristalsis, intestinal flora imbalance and weakened immunity with increasing age [21]. The age of patients with deficiency of spleen-energy and stagnation of wetness-evil, and deficiency of yin-fluid and phlegm-wetness syndrome (average age was lower than 50 years old) was lower than that of other syndromes (average age was higher than 55 years old). This suggests that the patients younger than 50 years old should be paid more attention to invigorating the spleen and eliminating wetness-evil during determination of treatment based on the differentiation of symptoms and signs. While eliminating wetness, we should take care of nourishing yin fluid, and we should not use drugs that are too pungent and dry. The results of this study also found that the proportion of male patients was more than that of female patients, which is consistent with the results of big data analysis [22]. It may be that men prefer smoking and drinking, and work and life are more stressful than women.
In this study, we found that some patients with colorectal polyps were complicated with hyperglycemia, hypertension, hyperlipemia and hyperuricemia (4H). Whether these complicating disease are related to the formation of asthenia- and sthenia-syndrome of colorectal tumor? Although some studies have suggested that there was no direct correlation between the number of colonic polyps and hyperglycemia, hypertension and hyperlipidemia [23], a research by Yunfeng Dong shown that the high risk factors of adenomatous rectal polyps are eating fat and having high triglyceride/cholesterol [24]. Our research results also shown that, in the colorectal polyp patients with asthenia-syndrome, the asthenia of spleen and stomach, and deficiency of yin fluid in these with hyperuricemia accounted for a large proportion. Although the difference was not statistically significant, drugs for reducing uric acid can be complemented each other while invigorating vital energy and spleen and nourishing yin fluid for such patients in clinic.
In view of the recurrence of colorectal polyps, based on the theory of insidious toxin (a pathogenic factors) in Traditional Chinese Medicine, some studies suggest that the primary cause of colorectal polyps is that the insidious toxin deeply invaded the intestinal collaterals. Therefore, the insidious toxin and chronic consumption of essence and blood are the key mechanisms of occurrence and recurrence of colorectal polyps [25], which indicates that toxic evil is also a pathological factor in the occurrence of intestinal polyps. In our study, we found that the patients with wetness-heat or phlegm-heat evil also accounted for a large proportion, while the patients with cold-wetness only accounted for a small proportion, which may be related to the unique climate environment in Shenzhen. Therefore, invigorating spleen, clearing away heat and eliminating wetness has become a strategy to prevent and treat colorectal polyps [26- 31]. Consistent with previous studies, it is easy to appear the syndrome of yin fluid deficiency because toxic and heat evil can consume essence and blood. As shown in our study, the syndromes of deficiency of yin fluid including yin-deficiency of liver and kidney, deficiency of stomach-yin, deficiency of lung-yin, and deficiency of both vital energy and yin also occupied a large proportion in the asthenia-syndrome. After statistical analysis, we found that there was no significant difference in the “4H” diseases between the patients with sthenia-syndrome, suggesting that there is no significant correlation between sthenia-syndromes and “4H” diseases.
Clinically, the occurrence of diseases is often presented by Asthenia-Syndrome Accompanied with Sthenia-Syndrome (ASASS), therefore, there are quite a few patients with the ASASS in this study. Among them, deficiency of vital energy and blood stasis was the major ones, followed by deficiency of spleen-energy and phlegm-wetness syndrome. Ultimately, asthenia is still rooted as the occurrence of intestinal polyps, with phlegm-wetness, blood stasis and stagnation of vital energy as the symptomatic manifestation, which is consistent with the treatment thinking of supplementing vital energy and invigorating the spleen, and promoting blood circulation and removing blood stasis to treat colorectal polyps [32]. A large number of studies have suggested that most patients with hypertension presented the syndrome of sthenia of liver-yang, and a significant correlation existed between the sthenia of liver-yang and hypertension [33-35]. Therefore, in this study, we also found that the difference of hypertension in the syndrome of ASASS was statistically significant. The proportion of patients with hypertension and sthenia of liver-yang was more than other syndromes, so it is necessary to pay attention to the prevention and treatment of hypertension in the therapy of colorectal polyp patients with sthenia of liver-yang.
Conclusion
Deficiency of vital energy of spleen-stomach and stagnation of phlegm-wetness are the primary syndromes for the patients with colorectal polyps in Shenzhen, and the pathological factors involve phlegm-wetness, blood stasis and stagnation of vital energy. Yin-deficiency is mainly caused by liver, kidney, lung and stomach. There is no obvious correlation between stheniasyndrome and age, sex, “4H”. Age should be considered in the treatment of patients under 50 years old with ASASS syndrome. The patients with sthenia of liver-yang syndrome often have hypertension, thus, hypertension should also be considered for such patients.
Declarations
Conflict of interest statement: All authors declare no conflict of interest.
Acknowledgement: This work was supported by National Natural Science Foundation of China (81903985).
References
- Zhang S, Sun K, Zheng E, et al. Cancer incidence and mortality in China, 2015. Journal of the National Cancer Center. 2021; 1: 2-11.
- Herszényi L. The “Difficult” Colorectal Polyps and Adenomas: Practical Aspects. Dig Dis. 2019; 37: 394-399.
- Wang KW, Dong M. Potential applications of artificial intelligence in colorectal polyps and cancer: Recent advances and prospects. World J Gastroenterol. 2020; 26: 5090-5100.
- Bailie L, Loughrey MB, Coleman HG. Lifestyle Risk Factors for Serrated Colorectal Polyps: A Systematic Review and Meta-analysis. Gastroenterology. 2017; 152: 92-104.
- He X, Wu K, Ogino S, Giovannucci EL, Chan AT, et al. Association Between Risk Factors for Colorectal Cancer and Risk of Serrated Polyps and Conventional Adenomas. Gastroenterology. 2018; 155: 355-373.e18.
- Fliss-Isakov N, Kariv R, Webb M, Ivancovsky-Wajcman D, Zaslavsky O, et al. A healthy lifestyle pattern has a protective association with colorectal polyps. Eur J Clin Nutr. 2020; 74: 328- 337.
- Erben V, Carr PR, Holleczek B, Stegmaier C, Hoffmeister M, et al. Strong associations of a healthy lifestyle with all stages of colorectal carcinogenesis: Results from a large cohort of participants of screening colonoscopy. Int J Cancer. 2019; 144: 2135- 2143.
- Mao Wenxin, Zhong Ziyou, Huang Suiping, et al. Analysis of Location of Colorectal Polyps and Characteristics of Traditional Chinese Medicine Syndromes. Journal of Guangzhou University of Traditional Chinese Medicine. 2020; 37: 818-822.
- Chinese medicine diagnostic branch of Chinese medicine association. Diagnostic criteria of common TCM syndromes (I). Journal of traditional chinese medicine university of Hunan. 2008; 28: 3-10.
- Zhou Zhongying. Internal Medicine of Traditional Chinese Medicine. Beijing: China Traditional Chinese Medicine Press. 2003.
- Yan Zaihong, Zhang Junying, Liang Huixia, et al. Epidemiological investigation of colorectal polyps among healthy people in Langfang area. Practical Preventive Medicine. 2016; 23: 1084-1085.
- Hu Denghua, Wen Guangxu, Kang Qingjie, et al. A Retrospective control analysis on effect and safety of HSP and CSP for treating of colorectal polyps. Chongqing medical. 2021; 50: 2013-2015.
- Chen Xuan, Xi Biao, Han Chunxia, et al. Retrospective analysis of TCM syndromes and integrative treatment of TCM and WM in 119 patients with colonic polyps. Inner Mongolia Journal of Traditional Chinese Medicine. 2019; 38: 143-144.
- Chu Yongqing, Chen Xia, Li Li, et al. Study on TCM syndrome types and TCM constitution distribution of 160 patients with colorectal polyps. Journal of Traditional Chinese Medicine. 2021; 62: 966-970.
- Zhao Hongbo, Wu Xiaojing, Yang Yun, et al. Correlation of endoscopic morphological characteristics and pathological types with traditional Chinese medicine syndrome types of colorectal polyps. World Chinese Journal of Digestology. 2020; 28: 1068-1075.
- Yang Wenge, Liao Jinling, Zhang Zhijie, et al. Study on the Pathological Types and Prognosis of Polyps in Patients with Blood Stasis Colorectal Polyps. Medical Information. 2020; 33: 93-95.
- Tate DJ, Desomer L, Klein A, Brown G, Hourigan LF, et al. Adenoma recurrence after piecemeal colonic EMR is predictable: the Sydney EMR recurrence tool. Gastrointest Endosc. 2017; 85: 647-656.e6.
- Yang Shanying, Guo Likun, Lu Chan, et al. A comparative study on the clinical characteristics of colorectal polyps between the elderly people and young and middle-aged people. Geriatrics and Health Care. 2021; 27: 85-89.
- Chen Z, Hu J, Zheng Z, Wang C, Lin D, Huang Y, et al. Location of colorectal adenomas and serrated polyps in patients under age 50. Int J Colorectal Dis. 2019; 34: 2201-2204.
- Segev L, Kalady MF, Plesec T, Mor E, Schtrechman G, et al. The location of premalignant colorectal polyps under age 50: a further rationale for screening sigmoidoscopy. Int J Colorectal Dis. 2020; 35: 529-535.
- Long Sidan, Ji Shuangshuang, Yao Shukun. Research progress on demographic characteristics and living habits of patients with intestinal polyps. Chin J Integr Trad West Med Dig. 2020; 28: 319-322.
- Yu Chunyue. Study on the distribution of TCM constitution types of patients with colorectal polyps. Beijing: Beijing University of Chinese Medicine. 2016.
- An Yu, Yu Xiaobing, Li Hongliang, et al. Investigation of risk factors for recurrence of colorectal adenomatous polyps after endoscopic treatment. Ningxia Med J. 2021; 43: 504-507.
- Dong Yunfeng, Guo Fengxia, Liu Xiaojuan, et al. Risk factors of colorectal adenomatous polyps among workers in Huabei Oil-field. Journal of Harbin Medical University. 2021; 55: 267- 270+277.
- Liang Baoyi, Zhang Beiping. Exploring the etiology and pathogenesis of colorectal polyps based on the theory of latent poison. International Journal of Traditional Chinese Medicine. 2020; 42: 1168-1171.
- Li Xiaolan, Yuan Gang, Zhu Junzhang, et al. Prevention of recurrence of colorectal polyps after endoscopic mucosal resection by invigorating spleen, clearing away heat and dampness. Chin J Integr Trad West Med Dig. 2021; 29: 460-463.
- Guo Haijun, Guo Xiuxia, Wang Benxian. Clinical Study on Jianpi Xiaoji Qingre Method in Preventing and Treating Recurrence of Colorectal Adenomatous Polyps. J New Chinese Medicine. 2020; 52: 66-69.
- Ao Li-yuan, Li Shiqi. Treatment of 30 cases of symptoms after resection of colorectal polyps with damp-heat retention. Fujian Traditional Chinese Medicine. 2018; 49: 87-88.
- Xie Fei, Luo Qinghua, Zhu Qunhui. Efficacy of Qingre Huashi Changning Decoction on Inflammatory Colon Polyps Patients with Damp and Hot Accumulate Spleen Syndrome. Journal of Emergency in Traditional Chinese Medicine. 2015; 24: 864-865.
- Tao Yuan, Wang Chunyan, Wei Wang, et al. Analysis on the medication rule of traditional Chinese medicine in the prevention of recurrence of colorectal polyps after operation. Chinese Medicine Modern Distance Education of China. 2020; 18: 58-61.
- Jin Jian, Zhang Xiang ‘an, Haixia Guo, et al. Professor Zhang Dongyue’s experience in treating colorectal polyps with Xinyunling recipe. Research of Traditional Chinese Medicine. 2020; 33: 39-41.
- Huo Long, Sun Shenwei, Gong Yuping, et al. Retrospective study of modified Xiaotan Decoction in the prevention of polyp recurrence after colorectal polypectomy (spleen deficiency with blood stasis syndrome). Shanghai Journal of Traditional Chinese Medicine. 2017; 51: 48-50.
- Yi Wuqiang, Cai Shufang, Cai Xuyang. Curative effect analysis of Tianma Gouteng Decoction combined with western medicine on hypertension with hyperactivity of liver yang. Clinical of Integrated Traditional Chinese and Western Medicine. 2021; 21: 123-124+140.
- Sun Lingling, Zhangyan. Research progress of treating hypertension by calming liver and suppressing yang. Journal of Practical Traditional Chinese Internal Medicine. 2021; 35: 55-57.
- Hao Ji-Xiang, Zhang Hong-ye, Xiong Kai-Peng, et al. A randomized parallel controlled study of Tianma Gouteng Granule combined with felodipine tablets in the treatment of hypertension. Journal of Practical Traditional Chinese Internal Medicine. 2020; 34: 100-102.