
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A new diagnostic paradigm for Erythromelanosis Follicularis Faciei et Colli: Dermoscopic and reflectance confocal microscopic features
Laura Diluvio*; Valeria Manfreda; Arianna Piccolo; Caterina Lanna; Elena Campione; Luca Bianchi
Dermatology, Department of Systems Medicine, University of Rome Tor Vergata, Viale Oxford, 81 00133 Rome, Italy
*Corresponding Author: Laura Diluvio
Department of Dermatology, University of Rome
“Tor Vergata” Viale Oxford, 81 – 00133 Rome, Italy.
Email: [email protected]
Received : Jan 25, 2022
Accepted : Mar 17, 2022
Published : Mar 24, 2022
Archived : www.jcimcr.org
Copyright : © Diluvio L (2022).
Abstract
Introduction: Erythromelanosis Follicularis Faciei et Colli is a rare variant of Kerastosis pilaris, characterized by a clinical triad of erythema, hyperpigmentation and follicular papules involving bilaterally cheeks, preauricular and maxillary areas of young male or, more rarely, female patients
Case presentation: A 21-year-old Caucasian woman presented symmetrical patches of hyperpigmentation, erythema with microscopic telangiectasias and tiny follicular papules involving cheeks, preauricular and maxillary areas, forehead, pinna and neck since childhood. Lesions were asymptomatic but caused profound cosmetic disfigurement and had a negative impact on her social life. The patient underwent a non-invasive diagnostic procedure with epiluminescence and confocal microscopy. Dermoscopic examination revealed prominent yellowwhitish follicular keratotic plugging over a reddish background with short fine telangiectasia in the perifollicular and interfollicular areas. Furthermore, RCM features displayed the presence of enlarged the presence of enlarged follicular openings, absence of demodex mites within the follicles and slight infundibular hyperkeratosis. At the level of the epidermal-dermal junction hyperpigmentation of the epithelial basal cell layer and dilation of dermal capillaries inside dermal papillae were observed, correlating to typical histological features of EFFC. Our patient benefited from the topical use of tretinoin 0.05% cream, with attenuation of the instrumental pictures.
Conclusion: Characteristic plugging over a reddish background and morphological features revealed by RCM may be helpful for assessment and monitoring in patients with EFFC. Starting from the observation of this case we would like to underline the importance of a noninvasive diagnostic procedure and an effective therapy for such a rare condition.
Keywords: Erythromelanosis Follicularis Faciei et Colli; Erythromelanosis Follicularis Faciei diagnosis; Dermoscopy; In vivo reflectance confocal microscopy.
Abbreviations: EFFC: Erythromelanosis Follicularis Faciei et Colli; EFF: Erythromelanosis Follicularis Faciei; RCM: Confocal Microscopy
Citation: Diluvio L, Manfreda V, Piccolo A, Lanna C, Campione E, et al. A new diagnostic paradigm for Erythromelanosis Follicularis Faciei et Colli: Dermoscopic and reflectance confocal microscopic features. J Clin Images Med Case Rep. 2022; 3(3): 1756.
Introduction
Erythromelanosis Follicularis Faciei et Colli (EFFC) represents an infrequently diagnosed condition of the pilary follicle that mainly affects children or adolescents, with a higher incidence in Asians [1]. EFFC was initially reported in young male patients, but a recent study showed nearly equal incidence between males and females [2]. The etiopathogenesis remains elusive, although a genetic background with autosomal recessive inheritance, sporadic mutation, nervous dysfunction and sun exposure are probably implicated [3]. The acronym Erythromelanosis Follicularis Faciei (EFF) was coined by Kitamura to describe a well-defined triad of erythema, hyperpigmentation and follicular papules involving bilaterally cheeks, preauricular and maxillary areas [4]. More rarely, the neck is affected and the disease is called EFFC. Diffuse brown pigmentation may be missing, especially in fair skin types, while keratosis pilaris is frequently associated, as observed in our patient [1,4]. Photosensitivity, pruritus, xerosis, and atopic dermatitis can be associated with this rare condition [2]. We report a morphological description in a patient affected by EFFC via non-invasive procedures, dermoscopy and confocal examination, avoiding the need for a biopsy in a visible skin area and to redefine the diagnosis and monitor the therapy.
Case presentation
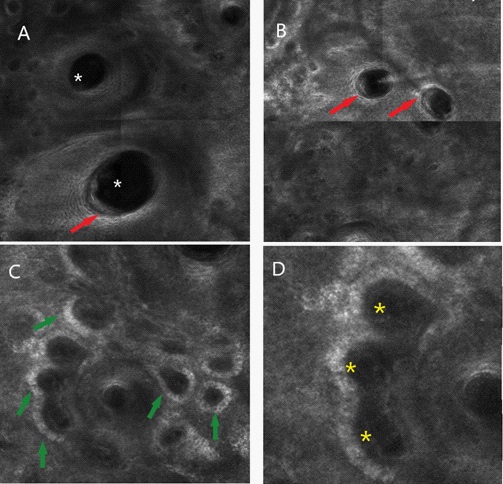
A 21-year-old Caucasian woman with Fitzpatrick skin type II was referred to our Dermatological Unit for facial skin lesions that have been presented since she was a child. Physical examination revealed symmetrical patches of hyperpigmentation, erythema with microscopic telangiectasias and tiny follicular papules involving the cheeks, preauricular and maxillary areas, forehead, pinna and neck, associated with an increased sebum production (Figure 1A,1B). A marked keratosis pilaris was noted at the upper trunk, especially on chest (Figure 1C). Lesions were asymptomatic but caused profound cosmetic disfigurement and had a negative impact on social life. Medical history was significant for a Hashimoto’s thyroiditis and a polycystic ovary syndrome treated with oral contraceptive therapy. Her family history was negative for similar skin disease. Polarized light dermoscopic evaluation of the cheeks revealed prominent yellowwhitish follicular keratotic plugging over a reddish background with short fine teleangectasia in the perifollicular and interfollicular areas (Figure 1d). The peppering observed by Errichetti and collegues was absent perhaps due to the skin phototype of the patient [5]. In accordance with this clinical and dermoscopic findings [5,6], we made the diagnosis of EFFC and decided to avoid incisional biopsy of the face, preferring to perform a confocal laser microscopic analysis. In vivo reflectance confocal microscopy (RCM) represents a non-invasive technique for in vivo microscopic visualization of the superficial layers of the skin up to 200 µm, with cellular-level resolution. RCM images revealed the presence of enlarged the presence of enlarged follicular openings, absence of demodex mites within the follicles and slight infundibular hyperkeratosis. At the level of the epidermal-dermal junction hyperpigmentation of the epithelial basal cell layer and dilation of dermal capillaries inside dermal papillae were observed. Our patient benefited from the topical use of retinoid, tretinoin at 0.05% cream, with partial resolution of erythema and follicular keratosis after eight weeks of treatment. After therapy, instrumental examinations revealed a reduction of follicular plugs over the reddish background under dermoscopy and decrease of follicular openings, infundibular hyperkeratosis, hyperpigmentation of epithelial basal cell layer and dilation of dermal capillaries observed by RCM (data not shown).
Discussion and conclusion
Erythromelanosis Follicularis Faciei et Colli is a rare variant of Kerastosis pilaris, that usually occurs between 8 and 12 years of age, characterized by a clinical triad of erythema, hyperpigmentation and follicular papules without skin atrophy or scarring. We present a 21-year-old Caucasian woman with symmetrical patches of hyperpigmentation, erythema with microscopic telangiectasias and tiny follicular papules involving the cheeks, preauricular and maxillary areas, forehead, pinna and neck, associated with an increased sebum production (Figure 1A,1B). A marked keratosis pilaris was noted at the upper trunk, especially on chest (Figure 1C). Lesions were asymptomatic but caused profound cosmetic disfigurement and had a negative impact on social life.

In our case, dermoscopic characteristics showed prominent yellow-whitish follicular keratotic plugging over a reddish background with short fine telangiectasia in the perifollicular and interfollicular areas. Furthermore, RCM highlights are related to the typical histological features of EFFC, showing follicular dilatation, mild follicular hyperkeratosis and hyperpigmentation of the epithelial basal cell layer are usually observed in the epidermidis, dilated blood vessels and lymphocytic perivascular infiltration mark the upper dermis [6,7]. The differential diagnosis encompasses atrophoderma vermiculatum, ulerythema ophryogenes, poikiloderma of Civatte, erythrose peribuccale pigmentaire of Brocq, Keratosis pilaris atrophicans faciei or lichen pilaris faciei, keratosis rubra pilaris, Riehl’s melanosis, acneform eruptions, and rarely Becker’s nevus [2,8]. So far, no treatment has proven satisfactory in the therapy of EFFC. Various options have been explored but lesions recur once the treatment is discontinued. Topicals keratolytic agents such as ammonium lactate (12%), tretinoin cream (0.05%, 1%), salicylic acid 2%, metronidazole, hydroquinone 4%, topical tacalcitol and chemical peel have been tried [6,7]. Intermittent oral isotretinoin and long-pulsed dye laser have been reported to be effective [2]. Avoidance of solar exposure and use of sunscreen is recommended. Characteristic plugging over a reddish background and morphological features revealed by RCM may be helpful for assessment and monitoring in patients with EFFC. Starting from the observation of this case we would like to underline the importance of a non-invasive diagnostic procedure and an effective therapy for such a rare condition.
Declarations
Conflicts of interest: No conflict of interest.
Authors Contribution Statement: Diluvio L. and Manfreda V. wrote the manuscript with input from all authors. Bianchi L. conceived the study. All authors discussed the results and commented on the manuscript.
Funding sources: No Funding sources
Data availability statement: Authors can confirm that all relevant data are included in the article and/or its supplementary information files
References
- Al Hawsawi K, Aljuhani O, Niaz G, Fallatah H and Alhawsawi A. Erythromelanosis Follicularis Faciei: A Case Report and Review of the Literature. Case Rep Dermatol. 2015; 7: 335-339.
- Rather S, Yaseen A and Mukhija M. Erythromelanosis Follicularis Faciei et Colli - A Cross-sectional, Descriptive study. Indian J Dermatol. 2016; 61: 308-313.
- Yanez, S, Velasco JA, and Gonzalez MP. Familial erythromelanosis follicularis et colli-an autosomal recessive mode of inheritance. Clin. Exp. Dermatol. 1993; 18: 283-285.
- Kitamura K, Kato H, Mishima Y and Sonoda S. Erythromelanosis follicularis faciei. Hautarzt. 1960; 11: 391-393.
- Errichetti E, Pizzolitto S and Stinco G. Dermoscopy of Erythromelanosis Follicularis Faciei et Colli. Actas Dermosifiliogr. 2017; 108: 779-781.
- Maouni S, El Anzi O, Sqalli A, Znati K, Meziane M and Hassam B. Erythromelanosis follicularis faciei et colli: Dermoscopy and dermatopathology correlates. JAAD Case Rep. 2019; 5: 535-536.
- Kim MG, Hong SJ, Son SJ, Song HJ, Kim IH, Oh CH and Moon JS. Quantitative histopathologic findings of erythromelanosis follicularis faciei et colli. J Cutan Pathol. 2001; 28: 160-164.
- Chakraborty S, Sil A, Bhanja DB. Follicularis faciei et colli Paediatr. Child Health 2020; 26: 133-134.