
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
“Milking” the way to diagnosis
Andreína Vasconcelos*; Bárbara Rodrigues; Pedro Ferreira
Centro Hospitalar do Baixo Vouga EPE, Aveiro, Portugal.
*Corresponding Author: Andreína Vasconcelos
Centro Hospitalar do Baixo Vouga EPE, Aveiro, Portugal.
Email: andreinavasconcelos03@gmail.com
Received : Mar 04, 2022
Accepted : Mar 18, 2022
Published : Mar 25, 2022
Archived : www.jcimcr.org
Copyright : © Vasconcelos A (2022).
Citation: Vasconcelos A, Rodrigues B, Ferreira P. “Milking” the way to diagnosis. J Clin Images Med Case Rep. 2022; 3(3): 1759.
Description
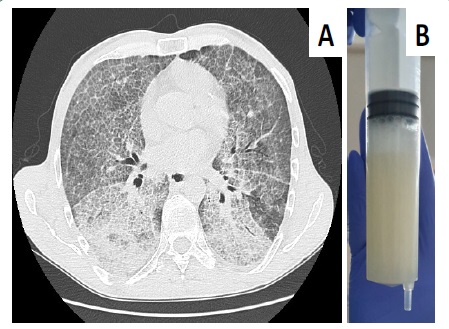
A 43-year-old non-smoker man presented to the emergency department with exertional dyspnoea and left pleuritic pain for 3 days. He denied fever or cough. He had history of pulmonary embolism, deep venous thrombosis and multiple opportunistic infections. At presentation, his oxygen saturation was 94% with venturi mask at 31% and lung auscultation showed basal crackles. He had no signs of peripheral oedema or deep venous thrombosis. Inflammatory parameters were within normal range. High-resolution chest computed tomography showed diffuse ground-glass opacities with interlobular and intralobular septal thickening — a pattern described as “crazy paving” (Panel A). Bronchoscopy yielded milky appearing lavage fluid (Panel B) and pathological testing revealed proteinaceous material positive on periodic acid–Schiff staining. These findings confirmed a diagnosis of pulmonary alveolar proteinosis (PAP). He underwent volume lavage of both lungs sequentially. At 6-month follow-up, he still maintained substantial improvement, with oxygen saturation of 94% in ambient air. PAP is a rare pulmonary disease caused by impaired surfactant turnover [1]. Although the crazy paving pattern is often associated with PAP [1], it’s not specific and can be seen in other conditions, including acute respiratory distress syndrome, pulmonary haemorrhage, organizing pneumonia, lipoid pneumonia and infections like Pneumocystis jirovecii [2] and SARS-CoV-2 pneumonia.
References
- Borie R, Danel C, Debray MP, Taille C, et al. Pulmonary alveolar Proteinosis. Eur Respir Review. 2011; 20: 98-107. DOI: 10.1183/09059180.00001311
- Radiopedia.org. 2020. Crazy Paving | Radiology Reference Article | Radiopedia.org | [online]. Available at: http://radiopedia.org/articles/crazy-paving [Accessed 3 June 2020]