
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
Transbiliary embolization of an iatrogenic porto-biliary fistula, a challenging complication
Joana Valcarcel José*; Daniel Pittí Freiburghaus; Albert Castillo Pinar; Jonathan R Joudanin Seijo
Radiology Department, Hospital Universitari de Bellvitge, 08907 Barcelona, Spain.
*Corresponding Author: Joana Valcarcel José
Departamento de Radiología, Hospital Universitario
de Bellvitge, Universidad de Barcelona, Barcelona,
España.
Email: jvalcarcel@bellvitgehospital.cat
Received : Feb 23, 2022
Accepted : Mar 23, 2022
Published : Mar 30, 2022
Archived : www.jcimcr.org
Copyright : © José JV (2022).
Abstract
Portobiliary fistulas are a rare complication of percutaneous transhepatic biliary procedures that could result in hemorrhage or sepsis. Hence we present a case of a transhepatic biliary drainage insertion in a patient with an underlying Bismuth type IV cholangiocarcinoma which resulted in a portobiliary fistula. Portobiliary fistula management is controversial. Moreover, to the best of our knowledge, there are few cases in the English literature reporting successful treatment. This case was successfully managed by controlled transbiliary embolization of a portal branch without compromising the main portal vein or bile ducts.
Keywords: Biliary procedures; Cholangiocarcinoma; Embolization; Complications.
Abbreviations: CT: Computed Tomography; MRI: Magnetic Resonance Imaging; PTBD: Percutaneous Transhepatic Biliary Drainages
Citation: Joana VJ, Daniel PF, Albert CP, Jonathan RJS. Transbiliary embolization of an iatrogenic porto-biliary fistula, a challenging complication. J Clin Images Med Case Rep. 2022; 3(3): 1766.
Introduction/background
Cholangiocarcinoma represents 2% of all cancer-related deaths worldwide and is the second most common cause of primary hepatic neoplasia (intrahepatic cholangiocarcinoma) [1]. Its evolution is usually insidious, which leads to a delayed diagnosis in advanced stages (stages II-IIIa-b or IV of the BismuthCorlette classification) [1]. Therapeutic options are usually limited, with only the surgical treatment being curative. Whether with curative or palliative intent, patients benefit from bile duct drainage. When the retrograde approach is not feasible or high bile duct occlusions are involved, percutaneous transhepatic cholangiography is an excellent alternative [2]. This approach is usually safe and effective in expert hands, but it is not exempt from possible complications (cholangitis, abscess, hepatic laceration, active bleeding, fistulas) [3]. Some of these complications are easy to solve (antibiotic therapy), although others, such as fistulas that compromise the biliary ducts, can bring real headaches to clinicians [3].
Case presentation
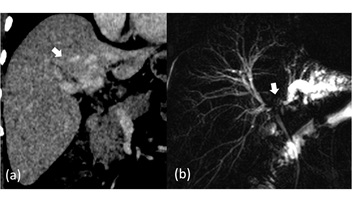
We report the case of a 35 years old male with painless cholestatic jaundice and weight loss, in whom a CT scan and MRI showed a hepatic hilum mass with bilateral intrahepatic bile ducts dilatation, suggesting a Cholangiocarcinoma - Klatskin tumor (Bismuth type IV) (Figure 1) and hilar lymphadenopathy. An endoscopic ultrasound fine-needle puncture was performed, which discarded metastatic nodal disease.
The multidisciplinary team (surgery, hepatology, oncology, radiology and interventional radiology) decided he was eligible for neoadjuvant chemotherapy, resection and liver transplantation.
In order to start oncological treatment and to optimize the patient for future surgery (cholestasis parameters), drainage of the bile ducts was required. A percutaneous transhepatic cholangiography was performed. We decided to drain the right lobe only because the left lobe was atrophic. It was necessary to place two internal-external PTBD (anterior and posterior radicles).
Forty-eight hours after the procedure, he presented great pain with the routinary flushing of one of the drainages. X-rays depicted a partial withdrawal of both drainages, and spontaneous hematic outflow was evident through the painful one.
The patient underwent fluoroscopic drainage revision and biliary endoprosthesis colocation, appreciating copious blood outflow during the replacement of the problematic drainage. In addition, cholangiography revealed the presence of a considerable porto-biliary fistula in relation to parenchymatous laceration (Figure 2a).
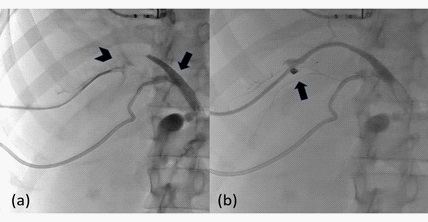
Given the risk of biliary occlusion and portal sepsis, we decided to carry out transbiliary embolization of the portal branch responsible for the fistula, proximal to the point of communication with the bile duct, using an Amplatzer-type 4 vascular occlusion device (6 mm) and coils (Figure 2b) The cholangiographic result was satisfactory with no evidence of fistula and cessation of blood externalization through the access. A CT performed later confirmed portal permeability.
Discussion
Biliary fistulas can be problematic and quickly become chronic (especially skin biliary fistulas). In the presence of a high-output fistula, it is prudent to perform an abdominal CT angiography to rule out arterial injury (pseudoaneurysm) [4], a candidate for endovascular embolization [5]. On other occasions, it is common to find the patient in the operating room undergoing a drainage review, as in the presented case, with the most common finding being the venobiliary fistula. The venobiliary fistula usually resolves spontaneously, requiring the placement of larger caliber drainages on certain occasions to promote hemostasis. Portobiliary fistulas are rare and controversial in their treatment [6]. Options for its management are often conservative, with a larger gauge drain placement. However, as it is a higher-pressure system than the central venous one, this measure may not be sufficient to achieve hemostasis so embolization may be necessary [7]. The most commonly used technique is retrograde embolization of the tract, conditioning a distal occlusion of the affected portal branch [8]. However, this technique does not allow the safe treatment of larger-caliber, central, and higher-debit fistulas. With the technique described in this case, controlled embolization is guaranteed while ensuring portal patency, being able to treat more central fistulas without conditioning non-target embolization. In conclusion, transbiliary embolization of a portobiliary fistula is safe and feasible without compromising the main portal vein branches or bile ducts.
References
- Banales JM, et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat Rev Gastroentero. 2020; 17: 557–588.
- Pomerantz BJ. Biliary Tract Interventions. Techniques Vasc Interventional Radiology. 2009; 12: 162–170
- Winick AB, Waybill PN, Venbrux AC. Complications of percutaneous transhepatic biliary interventions. Techniques Vasc Interventional Radiology. 2001; 4: 200–206.
- Hurtarte Sandoval AR, Flores Robles BJ, Penate Dardón JD, González Galilea Á. Haemobilia due to iatrogenic portobiliary fistula after cholecystectomy. Bmj Case Reports. 2013; bcr2013009768.
- Nakagawa N, Nakajima Y, Bird SM, Wakabayashi M. Immediate transbiliary embolization of a biliary-hepatic artery fistula encountered during access for percutaneous biliary drainage. Cardiovasc Inter Rad. 1994; 17: 295–297.
- Stableforth WD, et al. Iatrogenic portobiliary fistula complicating endoscopic stenting of a pancreatic cyst, with possible carcinoma: A case report. Gastrointest Endosc. 2011; 73: 630–632.
- Lorenz JM, Zangan SM, Leef JA, Ha TGV. Iatrogenic Portobiliary Fistula Treated by Stent-Graft Placement. Cardiovasc Inter Rad. 2010; 33: 421–424.
- Chanyaputhipong J, Lo R, Tan B, Chow P. Portobiliary fistula: Successful transcatheter treatment with embolisation coils. Singap Med J. 2014; 55: e34-36.