
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Management of spastic diplegic cerebral palsy and periventricular leukomalacia in a preterm 2-year-old: A case report and review of the literature
Raphia K Rahman, MBS1#; Nicole Palin, BS2#; Robyn Murphy, MD3; Catherine A Mazzola, MD4#*
1 Rowan University School of Osteopathic Medicine, Stratford, New Jersey, USA.
2 University of Maryland, College Park, Maryland, USA.
3 Department of Radiology, Morristown Medical Center, Morristown, New Jersey, USA.
4 Department of Neurological Surgery, Rutgers New Jersey Medical School, Newark, New Jersey, USA.
#Authors contributed equally to this manuscript
*Corresponding Author: Catherine A Mazzola
Department of Neurological Surgery, Rutgers New
Jersey Medical School, 185 S Orange Ave, Newark,
NJ 07103, USA.
Email: cmazzola@njpni.com
Received : Mar 01, 2022
Accepted : Mar 25, 2022
Published : Apr 01, 2022
Archived : www.jcimcr.org
Copyright : © Mazzola CA (2022).
Abstract
Periventricular Leukomalacia (PVL) is the most frequent brain injury to be associated with Cerebral Palsy (CP), especially in preterm infants. Spastic diplegia, a movement disorder commonly seen in CP, is characterized by increased muscle tone and spasticity in the lower extremities. The authors present a case of a 2-year-old child with mild PVL and spastic diplegia CP, with identifying factors including preterm birth history, his present age, and increasing severity of symptoms overtime. Magnetic resonance imaging was significant for an abnormally increased periventricular signal consistent with mild PVL. Due to worsening symptoms of toe-walking, increased gait width, and spasticity of lower extremities, interventions were recommended. This case demonstrates the neurodevelopmental consequences of PVL and ischemic brain injury in a preterm infant, resulting in spastic diplegic CP. A comprehensive and up-to-date review of the literature on PVL and spastic diplegia associated with CP is explored.
Keywords: Cerebral palsy; Preterm; Spasticity; Hypoxic-ischemic encephalopathy; Magnetic resonance imaging.
Abbreviations: PVL: Periventricular Leukomalacia; CP: Cerebral Palsy; MRI: Magnetic Resonance Imaging; HIE: Hypoxic-Ischemic Encephalopathy; HUS: Head Ultrasound.
Citation: Rahman RK, Palin NBS, Murphy R, Mazzola CA. Management of spastic diplegic cerebral palsy and periventricular leukomalacia in a preterm 2-year-old: A case report and review of the literature. J Clin Images Med Case Rep. 2022; 3(4): 1772.
Introduction
In the premature brain, ischemia-induced brain injuries may lead to significant neuro developmental impairments in children [1]. Periventricular Leukomalacia (PVL) is the most common type of ischemic brain injury of white matter observed in preterm infants, especially those born before 36 weeks’ gestation [2]. Perinatal asphyxia, or Hypoxic-Ischemic Encephalopathy (HIE) (i.e., inadequate oxygenated blood flow to the cerebral brain) causes perinatal damage to the cerebral cortex [2,3]. This activates microglial cells, which induces death of immature oligodendrocytes, resulting in white matter necrosis near the ventricles [3]. Severe white matter damage can lead to a secondary injury and cause a cascade of metabolic dysfunction which results in PVL [4]. Preterm PVL, caused by HIE, may be caused by premature rupture of membranes, intrauterine infection, or other causes of preterm labor [5]. This in turn disrupts proper myelination of axonal connections between essential developmental brain regions being formed during the last trimester of gestation (i.e., cerebellum and cerebral cortex) [4].
The authors present a case of a 2-year-old child with mild PVL and spastic diplegia CP, with identifying factors including preterm birth history (born at 32 weeks’ gestation), his present age, and increasing severity of symptoms overtime. Specifically, he exhibits worsening toe-walking with an increased width of toe usage and stiffness of the lower extremities. MRI results were significant for a mild abnormally increased periventricular signal consistent with mild PVL. This case thus highlights the neurodevelopmental consequences of PVL and ischemic brain injury in a preterm infant, resulting in spastic diplegic CP.
Early treatment of spasticity with appropriate management will ultimately prevent the development of contractures and permanent disability. It is critical for pediatricians, pediatric neurologists, and developmental pediatricians to be cognizant of pharmacologic treatments for spasticity in children that may require future neurosurgical intervention. Due to the patient’s age of 26 months, neurosurgical interventions such as selective dorsal rhizotomy or baclofen pump were discussed as options for the future. Thus, conservative management until permanent solutions are achieved is reviewed in this case. Additionally, a comprehensive and up-to-date review of the literature on PVL and cerebral palsy is presented.
Methods
Search strategy
A comprehensive literature search was performed to identify the most up to date publications about Periventricular Leukomalacia (PVL) and Cerebral Palsy (CP) in children (by authors R.R. and N.P.). We searched the PubMed database from December 2018 until May 2021 to identify relevant articles. Appropriate keywords and search terms used to identify all studies included: “periventricular leukomalacia” and “cerebral palsy” and “spastic diplegia” and “premature”. The reference lists of the final included articles were also searched to identify additional data sources. Inclusion criteria included literature specifically focused on PVL, CP, and spastic diplegia. A total of 9 articles extracted met inclusion criteria and were used for review.
Illustrative case report
Birth: The patient was born prematurely at 32 weeks’ gestation with APGAR (Appearance, Pulse, Grimace, Activity, and Respiration) scores of five at one minute and eight at five minutes, via emergency caesarean section due to premature rupture of membranes. During the perinatal period, the patient had respiratory distress syndrome and thus required continuous positive airway pressure therapy for three weeks. He additionally required phototherapy during the first week of life due to hyperbilirubinemia of prematurity which was resolved with treatment. He remained in the newborn intensive care unit for 2 months due to prematurity and apnea prior to being discharged.
Previous history: At 23 months of age, the child was evaluated by neurology for independently walking on his tiptoes and a bent knee on the left side. He was noted to be delayed in gross motor skills including crawling and walking and began walking at 22 months of age with frequent falls. Neurological examination was remarkable for spasticity of the lower extremities and stiffness of the ankles bilaterally (left ankle worse than right ankle). Upon gait examination, he was noted to walk on the toes bilaterally with the extremities abducted, thus uniquely diverging from the typical spastic gait which generally includes adduction of the extremities. His stiff wide based gait was also noted to be slightly unusual for spasticity.
He was thus recommended to begin physical therapy (twice weekly) and was prescribed oral Baclofen (5 mg BID), which was later increased to 5 mg in A.M. and 10 mg in P.M. Karyotype genetic testing and microarray were obtained due to global developmental delay with unrevealing results. There was also no familial history of neurological disease reported. A radiograph of the pelvis revealed well seated hips with no acetabular dysplasia. He was additionally recommended to begin wearing bilateral hinged Ankle-Foot Orthoses (AFOs) full-time during the daytime for contracture, stiffness, and plantar flexion of the ankles. The possibility of administering Botox injections in the future and serial casting was additionally addressed.
At 25 months of age, he was re-evaluated by neurology for frequent falls and ambulating with a bent left knee. Speech delay was diagnosed, and weekly speech therapy was started. Baclofen was tapered (to 5 mg PO BID for two weeks) due to unfavorable side effects reported by the mother, including irritability, lethargy, dizziness, fatigue, no relief of symptoms during the nighttime, and concerns that it may have contributed to unsteadiness. Continuation of physical therapy was recommended, along with a Magnetic Resonance Imaging (MRI) of the brain.
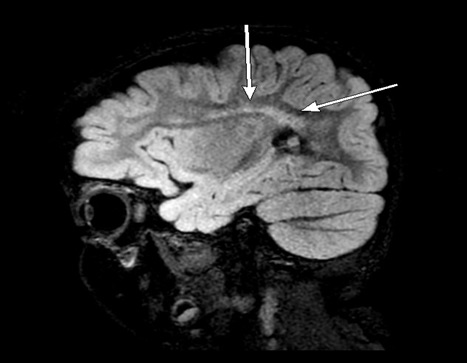
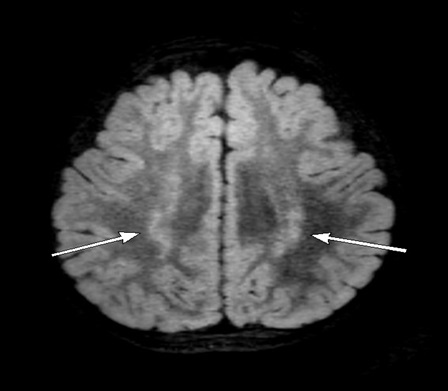
MR study: Multiplanar multisequence MR imaging of the brain pre- and post-contrast using gadobutrol 2 mmol/2 ml intravenous solution (1.5 mL administered) was obtained under anesthesia. Sagittal (A) and axial (B) T2 Fluid Attenuated Inversion Recovery (FLAIR) MR images showed some high signal in the centrum semiovale and corona radiata, which was more prominent posteriorly (Figures 1 and 2). A mildly abnormally increased periventricular signal was noted to be consistent with mild Periventricular Leukomalacia (PVL), with some degree of underlying gliosis suspected. No intracranial mass, hemorrhage, or hydrocephalus was evident.
Presentation: The child was referred for evaluation by our Neurosurgical team for increased toe-walking. His toe-walking was reported to worsen in severity overtime with an increased width of toe usage and stiffness of the lower extremities. He had no symptoms of urinary or bowel incontinence. During motor examination, spastic diplegia was evident with ⅘ strength in the right and lower extremities. Motor strength in the right and left upper extremities were 5/5. On Ashworth Spasticity Scale, there was ⅘ spasticity in the plantar flexors bilaterally. On sensory examination, he was able to discriminate between sharp and soft objects throughout. During gait examination, he had independent but abnormal ambulation, with the toes noted to turn inward during ambulation and abnormal coordination. Cranial nerves 2 through 12 were grossly intact. No scoliosis was noted. Head circumference was 48.49 centimeters (38%).
Management: Brain MR imaging results were reviewed by our institution. After evaluation, baclofen (5 mg in A.M. and 10 mg BID) was again recommended due to spastic diplegia with tightness of the plantar flexors bilaterally. Botox injections were also recommended for spasticity. The parents were extensively educated about the indications and benefits of Botox. Use of AFOs or construction boots were endorsed to keep the ankles in neutral position and to discourage the patient from toe-walking. Continuation of physical therapy (twice weekly) with the incorporation of stretching ten times daily was encouraged, and a referral was given for follow-up in 2 to 3 months at a center for cerebral palsy and spasticity. Neurosurgical interventions such as a selective dorsal rhizotomy or baclofen pump were not recommended during this initial consultation due to the patient’s age of 26 months. Those treatments were discussed as options for future, more permanent interventions.
Discussion
Children born with preterm PVL frequently demonstrate neurodevelopmental challenges such as visual, neurological, cognitive, and motor impairments, which can further be diagnosed as Cerebral Palsy (CP) [1]. In fact, preterm PVL lesions are the primary cause of CP symptomatology [4,6]. The most common clinical representation of a preterm child with CP and PVL is spastic diplegia, a subtype of CP [7,8]. Children affected with spastic diplegia CP may present with increased muscle tone and spasticity (i.e., stiffness or tightness of muscles and exaggerated reflexes) observed in the bilateral lower or upper extremities [9]. As discussed earlier, PVL pathogenesis disrupts the maturation and connections of essential brain regions. In the case of spastic diplegia CP, damage to neural pathways near the lateral ventricles can disrupt communication with the spinal cord and impair regulation of voluntary movement, causing spasticity [9]. Other signs and symptoms also found on presentation include delayed motor or movement milestones, toe-walking, abnormal or “scissored” gait, and impaired non-verbal intelligence, visuo-perceptual, and visuo-spatial abilities [7,9].
The most frequent motor disturbance reported in CP patients is spasticity, with spastic CP occurring in 78 to 87% of cases [10]. There is no current consensus among clinicians in the assessment of phenotype and motor disturbances in CP patients, therefore making it difficult to classify CP subtypes [11]. CP patients may display more than one type of motor disorder, and due to clinical variability, dystonia and choreoathetosis, may not be as easily recognized as spasticity [10]. It may often be difficult to distinguish between lower limb spasticity and sustained dystonic muscle contractions at rest [12]. In a retrospective study including 31 patients with CP in the setting of prematurity and PVL, it was found that the severity of dystonia, rather than spasticity, was associated with severity of motor functional disability, thus emphasizing the critical role of dystonia in motor functional disability [10]. Furthermore, a positive correlation was found to exist between the total dystonia score and severity of spasticity [10].
The most common clinical subtype of CP in the west is spastic diplegia, and it is the second most frequent subtype in the developing world [13]. Most children with spastic diplegia are born prematurely with the neuropathological presence of periventricular leukomalacia [14]. In a study comparing the antecedent risk factors, clinical profile, and MRI findings of term versus preterm-born children with spastic diplegia, it was found that periventricular white matter injury was less common in term-born children, with term spastic diplegia differing both clinically and neuropathologically from preterm spastic diplegia [14]. Term spastic diplegia was significantly associated with cortical and subcortical involvement, symptoms of moderate to severe intellectual disability, global developmental delay, and epilepsy [14]. Term-born children are still at risk of developing periventricular white matter injury due to prenatal insults including hypoxic or inflammatory insults, intrauterine growth restriction, or perinatal events such as neonatal encephalopathy [15,16].
PVL in term-born children with spastic diplegia is associated with cortical-subcortical lesions and malformations which may result in cognitive impairment and epilepsy [17]. In contrast, preterm children with an isolated injury of white matter were associated with a lower probability of seizures [18]. This suggests that term-born children with PVL may have a more diffuse injury of white matter when compared to preterm children with PVL [14]. In both term and preterm infants, perinatal brain injury is the primary cause of cerebral palsy [19]. Structural MRI is the standard used to evaluate for brain injury in term and preterm infants with suspected brain injury apparent on ultrasound. It was found that Diffusion Tensor Imaging (DTI) and functional MRI obtained soon after birth are potential biomarkers to help predict CP in newborns with perinatal brain injury, thus facilitating early intervention to improve motor outcomes in infants at risk of CP [19]. Infants with perinatal brain injury and CP were shown to have reduced structural and functional connectivity within motor networks during the neonatal period when compared to infants with perinatal brain injury and normal motor outcomes [19].
Preterm infants are typically diagnosed with cerebral palsy between 18 to 24 months [20]. In a case study of a preterm infant with bilateral periventricular leukomalacia evident on MRI at term, early detection of CP was facilitated using MR Spectroscopy (MRS) and Diffusional Kurtosis Imaging (DKI) combined with motor assessment [20]. MRS brain metabolites (in frontal white matter) and DKI-derived low fractional anisotropy values (in cortical white matter tracts) were both associated with clinical deficits evident later in life including visual motor skills, task attention, and motor coordination [20]. Early detection of CP using a combination of neuroimaging and developmental testing prompted early referral to therapy and interventional services at 2 months of age, helping to improve functional outcomes such as self-care, mobility, and communication skills [20].
The cerebellum is involved in the coordination of motor activity through information exchange with the cerebrum via the superior and middle cerebellar peduncles [21]. Prior studies have demonstrated infarction, hemorrhage, and volume loss of the cerebellum in preterm infants with PVL and/or CP, but the association between cerebellar white matter injury and CP remains unknown [21]. In a study investigating characteristics of cerebellar peduncle injury in preterm infants with PVL and/ or CP using Diffusion Tensor Imaging (DTI) and tractography, it was found that infants with CP had injuries of the ascending tracts (including the superior cerebellar peduncles and sensory tract); additional injury of the middle cerebellar peduncles also increased the severity of CP [21]. When compared to infants with normal motor function, preterm infants with CP had superior cerebellar peduncle injury characterized by lower fractional anisotropy and higher apparent diffusion coefficient [21]. Superior quantitative tractography assessment with DTI parameters at term-equivalent age may thus be useful in predicting the risk of CP and motor function impairment in preterm children [21].
Periventricular leukomalacia is classified into three categories, including cystic PVL (focal neuronal necrosis which evolve to multiple cysts), non-cystic PVL (microcysts associated with glial scarring), and diffuse astrogliosis [22]. In a meta-analysis, it was found that PVL is significantly associated with increased risk of developing CP, both in cystic and non-cystic form [5]. In a study by Hou et al., cystic PVL was not found to be significantly associated with mental delay in preterm infants, with cerebral palsy rates of 67% among infants with bilateral cystic PVL, 50% in those with unilateral cystic PVL, and 3% in the absence of cystic PVL [23]. This demonstrates the association of cystic PVL with motor delay based on the hypothesis that the location of cystic PVL typically involves motor tract fibers, thus resulting in motor dysfunction [24]
Diagnosing PVL can be performed through neuroimaging techniques. Cranial or Head Ultrasound (HUS) may be used to detect cysts or hollow regions in the tissue of a young infant’s brain [25]. However, Magnetic Resonance Imaging (MRI) is considered the gold standard modality for the detection of PVL in cases of HIE [25,26]. MRI radiographic features to identify PVL include areas of hyperintensity of periventricular white matter on T2-weighted sequences [26]. However, utilizing neuroimaging to estimate the severity of the injury is difficult at term equivalent age in preterm infants since there is a lack of evidence to support imaging prior to age of 1 year, despite the early clinical onset and symptomologies of PVL and spastic diplegia CP [25,26].
In a study by Boxum et al., it was determined that infants with a very high-risk of CP and the presence of cystic PVL performed worse in fine-tuning of postural adjustments from an early age onwards when compared to infants without cystic PVL [27]. The diffuse white matter injury in cystic PVL results in impairment of second level postural control, with increased latency in the recruitment of neck flexor and thoracic extensor muscles [27]. These findings suggest that infants with cystic PVL may benefit from early intervention approaches including the provision of adequate postural support to compensate for postural deficits [27]. Sitting position training and the incorporation of adaptive seating systems for tasks that require a stable sitting position can help enable CP patients to perform goal directed actions such as eating and playing [27].
Approximately 60-70% of children with cerebral palsy have cerebral visual impairment due to posterior visual pathway dysfunction, including optic radiations, occipital cortex, and visual associative areas [4,28]. This may be since injury of brain regions which result in motor deficits of CP is also anatomically related to the brain regions responsible for visual perception [28]. Periventricular leukomalacia involves both the corticospinal tract and visual pathways, including the optic tracts, posterior thalamus, and optic radiations [29,30]. In a study investigating visuo-haptic transfer for object recognition in children with PVL and bilateral cerebral palsy, results showed that PVL children have poor performance compared to control with deficits in visual and haptic object recognition skills that eventually improves with age [31].
Executive functions include mental processes such as working memory which may be negatively affected in cerebral palsy including spastic diplegia [9]. The ability to quickly process, maintain, update, and inhibit information may be affected in spastic diplegia due to white matter associative fibers altering structural connectivity of the brain, including the anterior cingulate cortex in children with unilateral PVL [9]. Thinning of the anterior or middle corpus callosum in preterm spastic diplegia may impair attention and executive functioning [9]. Children with pre—term spastic diplegia may also have impairment of non-verbal intelligence, visuo-perceptual, and visuo-spatial abilities [9]. In a study by Di Lieto et al. investigating the effect of adaptive working memory training on the executive functioning and visuo-spatial skills in children with preterm spastic diplegia, training significantly improved working memory abilities, visuospatial sills, inhibition of automatic responses, and phonological processing [9]. There were no correlations found between training effects and clinical characteristics such as chronological and gestational ages, intelligence level, and gross motor functioning [9]. These results thus suggest that home-based working memory training should be integrated into rehabilitation for children with preterm spastic diplegia to improve executive function [9].
Although there is no known cure for PVL and/or spastic diplegia CP, there are effective treatment options and surgical interventions that may help to alleviate symptoms and improve a child’s quality of life [8]. In general, PVL and spastic diplegia feature a common gait abnormality that is described as “idiopathic toe-walking.” Although toe walking is frequently observed in children with and without cerebral palsy, the exact underlying mechanism is unknown. It is, however, understood that muscles from CP patients can be spastic and form contractures, which limit the range of motion [32]. This is often seen specifically in the calf muscles, which can lead to toe walking. An effective, yet temporary treatment option for toe-walking patients with CP and spastic diplegia is Botulinum toxin A, or Botox injections. Botox can be injected into the bilateral calf muscles to promote functional equinus, control spasticity, and improve gait function [32].
Oral medications, such as baclofen, are also utilized in treating spasticity and management of general tone [33]. Combining BTX and oral baclofen with custom orthotic devices (i.e., AFO’s or casting) and physical/occupational therapy can be effective in helping to loosen muscles, achieve heal-strike, build strength, and promote overall physical healing and wellness over-time, respectively [8,32]. Children with CP are candidates for surgical intervention between the ages of 4 and 10, however there is no general consensus on the exact age [9]. In instances with increased severe limb or leg deformities, children may be candidates for lower-limb alignment orthopedic surgery [9]. Additionally, older children with spastic diplegia may be helped by Selective Dorsal Rhizotomy (SDR), an irreversible neurosurgical procedure, or a baclofen pump, both of which are utilized to reduce lower extremity spasticity and improve related symptomatology [9].
Conclusion
PVL is the most frequent ischemic-induced, white matter brain injury associated with spastic diplegia CP in premature infants. In the present case report, the authors describe a case of a 2-year-old child with mild PVL, spastic diplegic CP and a history of prematurity with worsening toe-walking and spasticity of the lower extremities. Conservative management of this patient included continuation of physical therapy and stretching, baclofen, recommendation for Botox injections, and use of AFOs to discourage toe-walking. The findings from our upto-date literature review suggest that future incorporation of sitting position training, adaptive seating systems, and homebased working memory training alongside rehabilitation can help to improve child outcomes in the CP population. In cases of CP with spasticity under the age of three, it is critical for clinicians to utilize neuroimaging techniques (including DTI and MRI) and developmental testing to help predict CP in newborns with perinatal brain injury, thus facilitating early intervention to improve motor outcomes in infants at risk.
Disclosures
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Our institution does not require ethical approval for reporting individual cases or case series.
Verbal informed consent was obtained from a legally authorized representative (s) for anonymized patient information to be published in this article.
References
- Schneider J, SP Miller. Preterm brain Injury: White matter injury, Handb Clin Neurol. 2019; 162: 155–172.
- Rana L, et al. MR Imaging of hypoxic ischemic encephalopathy - Distribution Patterns and ADC value correlations, Eur J Radiol Open. 2018; 5: 215–220.
- Qiao L, et al. Neuronal injury and roles of apoptosis and autophagy in a neonatal rat model of hypoxia-ischemia-induced periventricular leukomalacia. Mol Med Rep. 2018; 17: 5940–5949.
- Tinelli F, Guzzetta A, Purpura G, Pasquariello R, Cioni G, et al. Structural brain damage and visual disorders in children with cerebral palsy due to periventricular leukomalacia. Neuroimage Clin. 2020; 28: 102430.
- Gotardo JW, N de FV, Volkmer GP, Stangler AD, Dornelles BB, et al. Impact of peri-intraventricular haemorrhage and periventricular leukomalacia in the neurodevelopment of preterms: A systematic review and meta-analysis. PLoS One. 2019; 14: e0223427.
- Franki I, et al. The relationship between neuroimaging and motor outcome in children with cerebral palsy: A systematic review - Part A. Structural imaging, Res Dev Disabil. 2020; 100: 103606.
- Sah AK, Balaji GK, Agrahara S. Effects of Task-oriented Activities Based on Neurodevelopmental Therapy Principles on Trunk Control, Balance, and Gross Motor Function in Children with Spastic Diplegic Cerebral Palsy: A Single-blinded Randomized Clinical Trial. J Pediatr Neurosci. 2019; 14: 120–126.
- Summers J, et al. Selective dorsal rhizotomy in ambulant children with cerebral palsy: An observational cohort study. Lancet Child Adolesc Health. 2019; 3: 455–462.
- MC Di Lieto et al. Adaptive Working Memory Training Can Improve Executive Functioning and Visuo-Spatial Skills in Children with Pre-term Spastic Diplegia, Front Neurol. 2020; 11: 601148.
- Papadimitriou I, Dalivigka Z, Outsika C, Scarmeas N, Pons R, et al. Dystonia assessment in children with cerebral palsy and periventricular leukomalacia. Eur J Paediatr Neurol. 2021; 32: 8–15.
- Eggink H, et al. Spasticity, dyskinesia and ataxia in cerebral palsy: Are we sure we can differentiate them? Eur J Paediatr Neurol. 2017; 21: 703–706.
- Meijer IA, Pearson TS. The Twists of Pediatric Dystonia: Phenomenology, Classification, and Genetics, Semin Pediatr Neurol. 2018; 25: 65–74.
- Singhi P, Saini AG. Changes in the clinical spectrum of cerebral palsy over two decades in North India-An analysis of 1212 cases. J Trop Pediatr. 2013; 59: 434–440.
- Jauhari P, Singhi P, Sankhyan N, Malhi P, Vyas S, et al. A Comparison of Spastic Diplegia in Term and Preterm-Born Children. J Child Neurol. 2018; 33: 5: 333–339.
- Lasry O, Shevell MI, Dagenais L, REPACQ Consortium. Cross-sectional comparison of periventricular leukomalacia in preterm and term children. Neurology. 2010; 74: 1386–1391.
- Miller SP, Shevell MI, Patenaude Y, O’Gorman AM, et al. Neuromotor spectrum of periventricular leukomalacia in children born at term, Pediatr Neurol. 2000; 23: 155–159.
- Koeda T, Suganuma I, Kohno Y, Takamatsu T, Takeshita K, et al. MR imaging of spastic diplegia. Comparative study between preterm and term infants. Neuroradiology. 1990; 32: 187–190.
- Carlsson M, Hagberg G, Olsson I, et al. Clinical and aetiological aspects of epilepsy in children with cerebral palsy. Dev Med Child Neurol. 2003; 45: 371–376.
- Merhar SL, et al. Neonatal Functional and Structural Connectivity Are Associated with Cerebral Palsy at Two Years of Age, Am J Perinatol. 2020; 37: 137–145.
- Gullion L, Stansell J, Moss H, Jenkins D, Aljuhani T, et al. The Impact of Early Neuroimaging and Developmental Assessment in a Preterm Infant Diagnosed with Cerebral Palsy, Case Rep Pediatr. 2019; 2019: 9612507.
- Hasegawa T, et al. Cerebellar peduncle injury predicts motor impairments in preterm infants: A quantitative tractography study at term-equivalent age. Brain Dev. 2018; 40: 743–752.
- Khwaja O, Volpe JJ. Pathogenesis of cerebral white matter injury of prematurity, Arch Dis Child Fetal Neonatal Ed. 2008; 93: F153-161.
- Hou W, Tang PH, Agarwal P. The most useful cranial ultrasound predictor of neurodevelopmental outcome at 2 years for preterm infants. Clin Radiol. 2020; 75: 278–286.
- Staudt M, Pavlova M, Böhm S, Grodd W, Krägeloh-Mann I, et al. Pyramidal tract damage correlates with motor dysfunction in bilateral Periventricular Leukomalacia (PVL). Neuropediatrics. 2003; 34: 182–188.
- Agut T, et al. Preterm white matter injury: Ultrasound diagnosis and classification. Pediatr Res. 2020; 87: 37–49.
- Franki I, et al. The relationship between neuroimaging and motor outcome in children with cerebral palsy: A systematic review - Part A. Structural imaging. Res Dev Disabil. 2020; 100: 103606.
- Boxum AG, et al. Development of postural control in infancy in cerebral palsy and cystic periventricular leukomalacia, Res Dev Disabil. 2018; 78: 66–77.
- Schenk-Rootlieb AJ, van Nieuwenhuizen O, van Waes PF, van der Graaf Y, et al. Cerebral visual impairment in cerebral palsy: Relation to structural abnormalities of the cerebrum, Neuropediatrics. 1994; 25: 68–72.
- Jacobson LK, Dutton GN. Periventric. 2000; 45: 1–13.
- Lanzi G, et al. Cerebral visual impairment in periventricular leukomalacia, Neuropediatrics. 1998; 29: 145–150.
- Purpura G, Perazza S, Cioni G, Tinelli F. Visuo-haptic transfer for object recognition in children with periventricular leukomalacia and bilateral cerebral palsy, Child Neuropsychol. 2019; 25: 1084–1097.
- Weidensteiner C, et al. Quantification and Monitoring of the Effect of Botulinum Toxin A on Paretic Calf Muscles of Children With Cerebral Palsy With MRI: A Preliminary Study, Front Neurol. 2021; 12: 630435.
- Multani I, Manji J, Hastings-Ison T, Khot A, Graham K, et al. Botulinum Toxin in the Management of Children with Cerebral Palsy. Paediatr Drugs. 2019; 21: 261–281.