
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Treatment of horizontal root fracture with bioceramic cement: Case report
Kamila Duarte de Sousa1; Robeci Alves Macêdo Filho2; Renata Correia Sotero Dália Torres2; Sandra A. Marinho3*
1 Endodontics Specialist, Americas’ Dentistry Institute (IOA)/Paraiba Dentistry Institute (IOP), Brazil.
2 Professor, Americas’ Dentistry Institute (IOA)/Paraiba Dentistry Institute (IOP), Brazil.
3 Professor, Dentistry Course, State University of Paraiba (UEPB), Campus VIII, Brazil.
*Corresponding Author: Sandra A Marinho
Dentistry Course, State University of Paraiba UEPB),
Campus VIII,Cel Pedro Targino Street sn, 58233-000,
Araruna, PB, Brazil.
Email: san_mar2000@yahoo.com.br
Received : Mar 07, 2022
Accepted : Mar 29, 2022
Published : Apr 05, 2022
Archived : www.jcimcr.org
Copyright : © Marinho SA (2022).
Abstract
Horizontal root fractures involve cementum, dentin and pulp tissues, comprising between 0.5 and 7% of trauma cases that affect the permanent dentition. This paper aimed to report a case of horizontal root fracture, without immediate care, resulting from a car accident. Patient presented tooth 11 with darkening, coronary fracture and mobility grade two, in addition to negative responses to cold sensitivity tests and vertical and horizontal percussion tests. Through imaging exams, a horizontal fracture line was evidenced, with a local radiolucency. The treatment instituted was performed 12 years after the accident and consisted of endodontic treatment of the coronary fragment and its sealing with BIO-C® REPAIR bioceramic cement. Prompt care, correct diagnosis and adequate management of the case are important for a good prognosis of horizontal fractures. In the case reported, the treatment occurred in a mediate way, which may compromise the case prognosis. Close monitoring is essential to determine whether the therapy used was successful. Currently, the patient is asymptomatic.
Keywords: Tooth injuries; Infection control; Dental; Dental pulp devitalization.
Citation: Sousa KDD, Filho RAM, Torres RCSD, Marinho SA. Treatment of horizontal root fracture with bioceramic cement: Case report. J Clin Images Med Case Rep. 2022; 3(4): 1776.
Introduction
Root fractures are defined as trauma involving cementum, dentin and pulp, comprising only 0.5 to 7% of all traumatic dental injuries that affect the permanent dentition [1]. Its highest incidence occurs in anterior teeth and is usually the result of a frontal impact in the region [2]. They can be classified according to the direction (horizontal or vertical), the number of fracture lines (single or multiple) and the affected root region (cervical, middle and apical).
Horizontal root fractures are characterized by the rupture of rigid structures of the root, dividing the tooth into two segments, apical and coronal, and may occur at any point of the root, however, they are more frequent in the middle third [3].
The diagnosis is based on tooth mobility, displacement of the coronary fragment, sensitivity to palpation over the root and also on the fracture line, requiring several radiographic incidences to detect the lesion [4].
Healing events that follow after a fracture can be: Healing with hard tissue deposition, which is the ideal type of healing. The pulp is intact at the fracture site, or slightly stretched. In this case, there is initial formation of a bone callus, which stabilizes the fracture, followed by cementum deposition, with the fragments union. Healing with deposition of connective tissue may also occur, in cases where the pulp has been ruptured or severely stretched in the fracture region. In bacteria absence, a process of revascularization of the coronary portion is initiated, while periodontal ligament cells occupy the fracture region, resulting in fragments union with the formation of connective tissue. Another event is the absence of healing in the region, due to infection at the fracture line, as the coronal portion of the fracture is contaminated, resulting in the formation of inflammatory granulation tissue between the fragments, generating their separation and increasing coronary mobility [1].
Initially, the treatment of horizontal root fractures consists of repositioning the coronary fragment, when it is dislocated, and immobilizing it with rigid containment. Endodontic intervention is indicated only when there is pulp necrosis, which happens, in most cases, only in the coronary segment, while the apical segment remains vital [5].
Bioceramic materials (result of the combination of calcium silicate and calcium phosphate) are being widely used in cases of root fracture, as they have adequate sealing capacity and biocompatibility, in addition to inducing the formation of a mineralized barrier in the peri-radicular tissues, by formation of hydroxyapatite, enabling the creation of an apical plug, resulting in a reduction in treatment time [6], with satisfactory results [7-9].
Thus, the present study aims to report a clinical case of horizontal root fracture in the middle third of a central incisor, with endodontic therapy and sealing with bioceramic repair cement.
Case report
A 32-year-old male patient complained of tooth darkening. During the anamnesis, he reported having suffered a car accident approximately 12 years ago, in which he fractured the tooth 11, and its extraction was indicated, but the patient refused. The patient reported not being a smoker or having chronic diseases.
Intraoral exam (Figure 1), tooth 11 presented a blackened color and presence of a coronary fracture, grade two mobility, absence of periodontal pocket and presence of reaction tissue in the gingiva, in the middle third of the root.

The tooth responded negatively to the cold sensitivity test, indicating pulp necrosis and also to horizontal and vertical percussion tests. Radiographic exam showed a horizontal radiolucent image in the middle third of the root, indicating the presence of a fracture (Figure 2). Such tests suggest the absence of healing of the fragments due to infection at the fracture line.

The tooth responded negatively to the cold sensitivity test, indicating pulp necrosis and also to the horizontal and vertical percussion tests. Radiographic examination revealed a horizontal radiolucent image in the middle third of the root, indicating the presence of a fracture (Figure 2). Such tests suggest the absence of healing of the fragments due to infection at the fracture line.
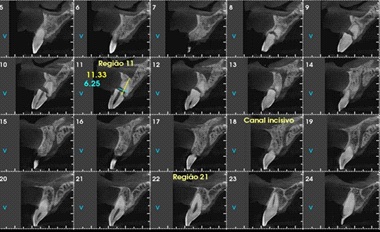
Cone beam computed tomography showed a horizontal hypodense image in the middle third of the root, with an oblique path in the vestibulo-palatal direction (Figure 3). Asymptomatic apical periodontitis was then diagnosed, associated with a horizontal root fracture in tooth 11.
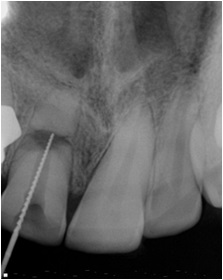
Endodontic treatment of the coronary third up to the fracture level was performed. After absolute isolation, access was performedwith irrigation and abundant chemical decontamination with Sodium Hypochlorite (NaOCl) 2.5%. Initial instrumentation was performed with #15 and #20 hand files and the working length was established using an electronic apex locator (Romiapex A 15, Romidan Dental QualityProducts, São Paulo, SP, Brazil), obtaining the measurement of 17mm incisal to the fracture region. This measurement was confirmed by radiographic odontometry (Figure 4).
Then, mechanized instrumentation was performed with Reciprocant R25 and R50 files (VDW, Munich, Germany). The final irrigation protocol was performed with mechanical agitation of the irrigant using motor-driven instruments with reciprocating motion, using the EasyClean (Easy Equipamentos Odontológicos, Belo Horizonte, Brazil), consisting of three 20-second agitation cycles with NaOCl, three stirring cycles of 20 seconds with liquid trisodium Ethylenediaminetetraacetic Acid (EDTA), and three more stirring cycles of NaOCl ethylenediaminetetraacetic acid.
After instrumentation and final irrigation protocol, excess moisture was removed from the interior of the canal with a sterile absorbent paper tip and the canal was filled with BIO®-C REPAIR cement (Angelus®, Maringá, Brazil). The periapical radiograph showed the filling of the entire canal extension (Figure 5). Shielding was performed with flow resin at the canal and filler resin in the coronal portion.
The patient was referred for an aesthetic reabilitation of tooth 11 and he is being followed up by the Service. He same signed a Free and Informed Consent Term.

Discussion
In cases of horizontal fractures, endodontic intervention should not be performed immediately, since the incidence of pulp necrosis is a little higher than 20% of cases [8], and clinical and radiographic follow-ups are indicated initially. The decision for endodontic therapy can be made after three months, in cases where the tooth does not respond to the cold sensitivity test and radiographs show radiolucency close to the fracture line
Immediate treatment of fractures in permanent teeth consists of fracture reduction and immobilization with rigid restraint [1], as the separation of the fragments is an important variable during fracture healing. If coronal fragment displacement is not severe, minimal damage to the pulp and periodontium will occur. However, when separating the fragments, repositioning must be performed for better healing [10]. In the present case, the patient did not undergo any treatment at the time of the accident, and the fracture was not reduced, disfavoring optimal healing and causing contamination at the fracture line [1].
When pulp necrosis develops, it is usually located in the coronary fragment, while apical segment remains vital. Therefore, endodontic treatment is indicated only in the coronary portion [9]. In the rare cases where both the coronary and apical pulp are necrotic, the apical segment must be surgically removed [5]. In complementary exams of the case reported, a radiolucent image was observed only in the fracture line region, suggesting pulp necrosis of the coronary fragment, which was confirmed by a sensitivity test. The treatment instituted, therefore, was endodontics of the coronary fragment and case follow-up.
In pulp necrosis cases, infection control is an important factor for repair to occur. Disinfection measures associated with the use of bioceramic cements to seal the coronary fragment show good results. Thus, to enhance the intracanal disinfection of the present case, mechanical agitation of the irrigant was performed, using instruments driven by motor with reciprocating movement, with EasyClean, a plastic instrument, which generates a vigorous agitation of the auxiliary chemical substances, promoting penetration of the irrigating solution in the lateral canals and providing better removal of the smear layer in the apical third, when compared to passive ultrasonic irrigation in an endodontic treatment [11,12].
Regarding the sealing of the coronary fragment, this will be more difficult, since there is no apical constriction. Calcium hydroxide has been used to favor the formation of this apical shield, however, it has disadvantages such as many sessions to change medication; the susceptibility of the canals to reinfection and the susceptibility to fracture of the treated roots [8]. The choice of a bioceramic as filling material for the coronary fragment is due to its proven physicochemical and biological properties. This material, in addition to presenting antimicrobial properties due to its alkaline pH, has a lower rate of microleakage (compared to calcium hydroxide) and does not compromise its sealing capacity in the presence of moisture, in addition to having the ability to induce osteogenesis and cementogenesis, favoring biological sealing [13]. So, the material of choice for the filling in the present case was BIO®-C REPAIR, a ready-touse bioceramic material. However, it has disadvantages, such as tooth color change and its difficult removal after accommodation of the material, which would make it difficult to remove it, in case of retreatment or preparation for an intraradicular post [14]. As the tooth in the present case already had a color change and the canal was meticulously filled, these disadvantages were temporarily overcome.
However, the prognosis of teeth with fractured roots will also be influenced by the location of the fracture line, the displacement of the fragments, and the pulp tissue and the patient’s general health conditions [5]. Follow-up may reveal problems in pulpal and periodontal healing, such as root canal obliteration and external and internal root resorption [1]. In the case reported, obliteration of the canal in the apical fragment could be observed.
Immediate care, correct diagnosis and adequate treatment are important for a good prognosis of horizontal fractures, with the need for follow-up in the first five years after treatment [3]. The present case still has a dubious prognosis due to the short follow-up time. However, the patient has not presented any symptoms so far and healing at the fracture line is awaited. The follow-up of horizontal root fracture treated with bioceramic cement (up to 10 years), has shown satisfactory results [7-9].
Conclusion
In cases of horizontal root fractures, treatment with bioceramic materials has been shown to be effective. In the clinical case reported, BIO®-C REPAIR was used to fill the coronary fragment. The healing at the fracture line is being awaited, with careful monitoring of the patient.
References
- Andreasen FM, Andreasen JO, Andersson MC. Textbook and Color Atlas of Traumatic Injuries to the Teeth. 2007. 4th Edition, Oxford: Blackwell.
- Mizuhashi F, Ogura I, Sugawara Y, Oohashi M, Mizuhashi R, et al. Diagnosis of root fractures using cone-beam computed tomography: Difference of vertical and horizontal root fracture. Oral Radiology. 2020; 37: 305-310.
- Teixeira BCS, Cerqueira JDM, Sardinha SCS, Carvalho ES. [Therapeutic approach rooth fracture with 30 months follow: clinical case report]. Rev. Odontol Bras Central. 2019; 28: 82-86. [In Portuguese] https://doi.org/10.36065/robrac.v28i85.1307
- Costa RBA, Coelho IWF, Carvalho FB, Crusoé-Rebello I, Neves FS, et al. [Clinical, radiographic and tomographic evaluation of root fractures: case series]. J Health Biol. 2019; 7: 172-176. [In Portuguese] doi: http://dx.doi.org/10.12662/2317-3076jhbs. v7i2.2332.p172-176.2019
- Duarte ALB, Silva MBM, Chagas KA, Silva CM, Santos JMB, et al. [Clinical Treatment of dental trauma: case report.] Brazilian Journal of Health Review. 2020; 3: 2581-2599. Available in: https:// www.brazilianjournals.com/index.php/BJHR/article/view/8254 [In Portuguese]. doi: https://doi.org/10.34119/bjhrv3n2-106
- Girelli CFM, Lima CO, Lacerda MFLS, Coellho RG, Silveira FF, et al. The importance of bioceramics and computed tomography in the late clinical management of a horizontal root fracture: A case report. J Clin Exp Dent. 2020; 12: e514-e518.
- Toscano MA, Zacharczuk GA, López GE. [Root fracture in the medium third: Treatment and 5 years follow up]. Rev Assoc Odontol Argent. 2019; 103: 103-109. [In Portuguese]
- Roig M, Espona J, Mercadé M, Duran Sindreu F. Horizontal root fracture treated with MTA, a case report with a 10-year followup. Dental Traumatology. 2011; 27: 460-463.
- Kim D, Yue W, Yoon TC, Park SH, Kim E, et al. Healing of Horizontal Intra-alveolar Root Fractures after Endodontic Treatment with Mineral Trioxide Aggregate. Journal of Endodontics. 2016; 42: 230-235.
- Andrade ES, Campos Sobrinho ALP, Andrade MGS, Matos JLF. Root healing after horizontal fracture: A case report with a 13- year follow up. Dent Dental Traumatology. 2008; 24: 1-3.
- Silva EJNL, Carvalho CR, Belladonna FG, Prado MC, Lopes RT, et al. Micro-CT evaluation of different final irrigation protocols on the removal of hard-tissue debris from isthmus-containing mesial root of mandibular molars. Clinical Oral Investigations. 2018; 23: 681-687.
- Kato AS, Cunha RS, da Silveira Bueno CE, Pelegrine RA, Fontana CE, de Martin AS. Investigation of the efficacy of passive ultrasonic irrigation versus irrigation with reciprocating activation: An environmental scanning electron microscopic study. J Endod. 2016; 42: 659-663.
- Oliveira JCM, Silva FSB, Pinto SSL. [Horizontal root fracture: case report]. Revista Brasileira de Odontologia. 2008; 65: 76-79. [In Portuguese]. doi: http://dx.doi.org/10.18363/rbo.v65n1.p.76
- Hess D, Solomon E, Spears R, He J, et al. Retreatability of a bioceramic root canal sealing material. J Endod. 2011; 37: 1547- 1549.