
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
A case of typical mycosis fungoides in an HIV-positive patient
Delice Kayishunge1; Sophia Ly1; Aadil Ahmed2; Henry K Wong2*
1 College of Medicine, University of Arkansas for Medical Sciences, USA.
2 Department of Dermatology, University of Arkansas for Medical Sciences, USA.
*Corresponding Author: Henry K Wong
Department of Dermatology, University of Arkansas
for Medical Sciences, USA.
Email: Hkwong@uams.edu
Received : Mar 08, 2022
Accepted : Mar 29, 2022
Published : Apr 05, 2022
Archived : www.jcimcr.org
Copyright : © Wong HK (2022).
Abstract
Non-Hodgkin’s lymphomas in HIV patients are generally B-cell lymphomas. The coexistence of HIV-1 infection with Cutaneous T-Cell Lymphoma (CTCL) is an infrequent occurrence, particularly in the classic variety of Mycosis Fungoides (MF). This case demonstrates that in an HIV-1 positive patient, CTCL can manifest as MF with features comparable to those reported in the general population. We report a 52-year-old male patient with asymptomatic HIV-1 who presented with the eruption of pruritic papules with overlying grey scales over his torso and extremities for two years. In a biopsy specimen, small intraepidermal lymphocytes without significant atypia were detected. Immunohistochemistry confirmed the diagnosis of T-cell lymphoma. The disease had spread to lymph nodes throughout the body. This is one of the few cases in which a typical MF is described in an HIV-1 patient. MF can be difficult to identify owing to its slow progression and resemblance to other inflammatory conditions such as spongiotic dermatitis. While MF is a very uncommon sign in HIV-infected individuals, it should be included in the differential diagnosis of all patients presenting with relevant cutaneous manifestations.
Keywords: Cutaneous T-cell lymphoma; Immunosuppression; HIV.
Citation: Kayishunge D, Ly S, Ahmed A, Wong HK. A case of typical mycosis fungoides in an HIV-positive patient. J Clin Images Med Case Rep. 2022; 3(4): 1778.
Introduction
Non-Hodgkin’s Lymphomas (NHL) are more common among patients with Acquired Immunodeficiency Syndrome (AIDS) than in the general population and occur in approximately 10% of all HIV-infected patients [1]. Most NHLs detected in AIDS patients are B-cell lineage and extranodal in origin, with primary sites in the gastrointestinal tract and central nervous system [2-4]. In comparison, cutaneous NHLs are a relatively uncommon occurrence in HIV-1-infected individuals. HIV-associated cutaneous lymphomas are predominantly T-cell lineage and classified into indolent diseases mimicking Mycosis Fungoides (MF) or Sezary syndrome or large cell lymphomas with a dismal prognosis, often CD30+ T-cell phenotype with Epstein-Barr virus positivity [5]. The majority of reported instances of Cutaneous T-Cell Lymphomas (CTCL) in HIV positive individuals resemble MF or Sezary syndrome [6-11,12-16]. Additionally, HIV positivity may operate as a protective factor against CTCL since HIVinfected patients have a better rate of survival and a lower risk of total mortality compared to non-HIV-infected CTCL patients [17]. We describe a case of MF in an HIV-positive patient who had typical MF features consistent with those observed in the general population.
Case presentation
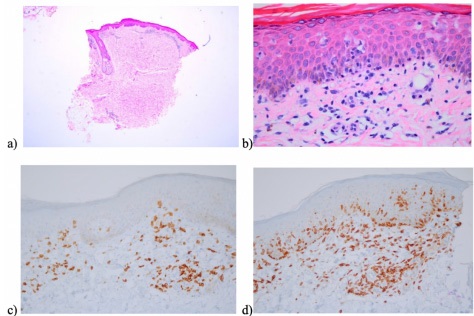
We report the case of a 52-year-old male patient with a history of asymptomatic HIV-1 infection who was referred for assessment of a rash and nonspecific skin eruption. When he arrived at our dermatology clinic, the patient felt good with no systemic symptoms but reported that these cutaneous symptoms began two years ago and progressively deteriorated. He stated that he had pruritus on his trunk and extremities, which he could alleviate by using baby oil. Clinical examination revealed a scattering of annular hypopigmented to mottled hyperpigmented macules, some with overlying scales, involving the arms, chest, abdomen, back, buttocks, and legs, against a background of scaly skin and increased skin lines on the chest, abdomen, back, and bilateral upper and lower extremities (Figure 1). The laboratory analysis consisted of an unremarkable Complete Blood Count (CBC), Comprehensive Metabolic Panel (CMP), and lipid panel. The patient previously had an asymptomatic HIV-1 infection, which was confirmed by serology testing. At baseline, the patient’s absolute CD3/CD4 helper T-cell count was 878/ uL, and he is not currently on antiretroviral therapy.

Clinical and pathological findings were consistent with mycosis fungoides stage 1B. Triamcinolone cream was begun on the patient with moderate control, so treatment was escalated to include full body NB-UVB three times a week. The treatment plan improved his rash and kept his labs well controlled.
Discussion
In comparison to the general population, individuals with HIV have an estimated 11-fold increased risk of developing malignant non-Hodgkin’s neoplasms [7]. Only a few of these neoplasms are T-cell lymphomas; the vast majority are B-cell lymphomas. CTCL can manifest itself in two ways in HIV-positive patients: as an indolent type mimicking mycosis fungoides or as an aggressive Sezary syndrome and large cell lymphoma. Goldstein et al. identified the first instance of localized CTCL in a patient infected with HIV-1. The patient had cutaneous tumors with no peripheral adenopathy or other indications of spreading. Local radiation treatment was used successfully to control the patient’s tumors [11]. Following that initial case, additional cases of CTCL in HIV-positive individuals have been described, in which patients present with aggressive lesions and a dismal prognosis [6-11,12-16].
Analysis of the Surveillance, Epidemiology, and End Results program, 1973–2013, of the US National Cancer Institute data showed that HIV-infected patients with CTCL have a significantly higher survival rate and a decreased risk of overall mortality than non-HIV-infected patients [17]. We herein report another rare case of mycosis fungoides with the typical features of indolent scaly patches that may or may not be irritating in an HIV-1 positive patient, as found in the general population. This case adds to the data that HIV may confer a protective status on the patient by destroying neoplastic T cells and that, in the absence of severe immunodeficiency, CTCL responds to standard therapy and progresses more slowly [8,17]. Notably, one of the primary goals of this case is to emphasize the critical nature of quick detection in such cases. The early stages of MF might be mistaken for non-cancerous inflammatory illnesses. Early biopsy of lesions may prevent a delay in diagnosis, averting the need for severe therapy later.
References
- Levine AM. Lymphoma in acquired immunodeficiency syndrome. Semin Oncol. 1990; 17: 104-112.
- Herndier BG, Friedman SL. Neoplasms of the gastrointestinal tract and hepatobiliary system in acquired immunodeficiency syndrome. Semin Liver Dis. 1992; 12: 128-141.
- Kaplan LD, Abrams DI, Feigal E, McGrath M, Kahn J, et al. AIDSassociated non-Hodgkin’s lymphoma in San Francisco. Jama. 1989; 261: 719-724.
- Nasr SA, Brynes RK, Garrison CP, Chan WC. Peripheral T-cell lymphoma in a patient with acquired immune deficiency syndrome. Cancer. 1988; 61: 947-951.
- Kerschmann RL, Berger TG, Weiss LM, Herndier BG, Abrahms KM, et al. Cutaneous presentations of lymphoma in human immunodeficiency virus disease. Predominance of T cell lineage. Arch Dermatol. 1995; 131: 1281-1288.
- Berger TG, Kerschmann RL, Roth R, Schulze K, Zackheim HS, et al. Sézary’s syndrome and human immunodeficiency virus infection. Arch Dermatol. 1995; 131: 739-741.
- Biggar RJ, Engels EA, Frisch M, Goedert JJ. Risk of T-cell lymphomas in persons with AIDS. J Acquir Immune Defic Syndr. 2001; 26: 371–376.
- Burns MK, Cooper KD. Cutaneous T-cell lymphoma associated with HIV infection. J Am Acad Dermatol. 1993; 29: 394-399.
- Crane GA, Variakojis D, Rosen ST, Sands AM, Roenigk HH, Jr. Cutaneous T-cell lymphoma in patients with human immunodeficiency virus infection. Arch Dermatol. 1991; 127: 989-994.
- Gahongayire F. Mycosis fungoides and Sezary syndrome against a human immunodeficiency virus-positive background: Case report. Int J Dermatol. 2007; 46: 32-35.
- Goldstein J, Becker N, DelRowe J, Davis L. Cutaneous T-cell lymphoma in a patient infected with human immunodeficiency virus type 1. Use of radiation therapy. Cancer. 1990; 66: 1130- 1132.
- Longacre TA, Foucar K, Koster F, Burgdorf W. Atypical cutaneous lymphoproliferative disorder resembling mycosis fungoides in AIDS. Report of a case with concurrent Kaposi’s sarcoma. Am J Dermatopathol. 1989; 11: 451-456.
- Muñoz-Pérez MA, Ríos-Martín JJ, Rodriguez-Pichardo A, Camacho F, et al. Cutaneous T-cell lymphoma and human immunodeficiency virus infection: 2 cases and a review of the literature. Acta Derm Venereol. 1999; 79: 153-155.
- Nahass GT, Kraffert CA, Penneys NS. Cutaneous T-cell lymphoma associated with the acquired immunodeficiency syndrome. Arch Dermatol. 1991; 127: 1020-1022.
- Zhang P, Chiriboga L, Jacobson M, Marsh E, Hennessey P, et al. Mycosis fungoides like T-cell cutaneous lymphoid infiltrates in patients with HIV infection. Am J Dermatopathol. 1995; 17: 29- 35.
- Zucker-Franklin D, Pancake BA, Friedman-Kien AE. Cutaneous disease resembling mycosis fungoides in HIV-infected patients whose skin and blood cells also harbor proviral HTLV type I. AIDS Res Hum Retroviruses. 1994; 10: 1173-1177.
- Wang J, Liang R, Hao C, Liu X, Zhang N, et al. Survival outcomes of primary cutaneous T-cell lymphoma in HIV-infected patients: a national population-based study. J Invest Med. 2018; 66: 762.