
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Garcin syndrome caused by rhino-orbito-cerebral mucormycosis
Ju Ying Chien1; Sung Yuan Hu1,2,3,4*; Ren Ching Wang5
1 Department of Emergency Medicine, Taichung Veterans General Hospital, Taichung, Taiwan.
2 School of Medicine, Chung Shan Medical University, Taichung, Taiwan.
3 Institute of Medicine, Chung Shan Medical University, Taichung, Taiwan.
4 Department of Post‐Baccalaureate Medicine, College of Medicine, National Chung Hsing University, Taichung, Taiwan.
5 Department of Pathology and Laboratory Medicine, Taichung, Taiwan.
*Corresponding Author: Sung-Yuan Hu
Department of Emergency Medicine, Taichung Veterans General Hospital, Taichung, Taiwan.
Email: song9168@pie.com.tw
Received : Mar 14, 2022
Accepted : Apr 01, 2022
Published : Apr 08, 2022
Archived : www.jcimcr.org
Copyright : © Sung-Yuan H (2022).
Abstract
Total paralysis of all or near all unilateral cranial nerves indicates Garcin syndrome. Garcin syndrome caused by Rhino-Orbito-Cerebral Mucormycosis (ROCM) complicating with cerebral infarction has been reported rarely. ROCM is an opportunistic fungal infection with high morbidity and mortality rates despite treatment due to acute angioinvasive infections. We report the case of a 69-year-old female, with a history of type 2 Diabetes Mellitus (DM), who presented Garcin syndrome caused by ROCM.
Keywords: Garcin syndrome; Multiple cranial nerve palsy; RhinoOrbito-Cerebral Mucormycosis (ROCM).
Abbreviations: CT: Computed Tomography; DM: Diabetes Mellitus; ROCM: Rhino-Orbito-Cerebral Mucormycosis.
Citation: Chien JY, Hu SY, Wang RC. Garcin syndrome caused by rhino-orbito-cerebral mucormycosis. J Clin Images Med Case Rep. 2022; 3(4): 1785.
Description
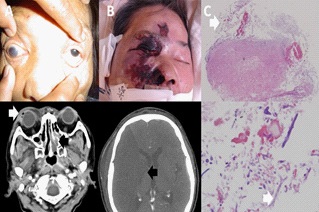
A 69-year-old DM female presented right ocular pain with diplopia and fever for 2 days. Neurological examination revealed dilated pupil of right eye with fixed gaze of right eye. CT showed mucus accumulation in paranasal sinus and gas bubbles in the right eyeball (Figure 1A). Two days later, eschar formation over rhino-orbital region with ptosis, impaired sensation, loss of nasolabial fold, absence of movement and sensation on palate and uvula, and deterioration of consciousness. Massive infarction of right middle cerebral artery and swollen scalp were detected on repeated CT (Figure 1B). Fungus culture from nostril yielded Rhizopus spp. Biopsy revealed angioinvasive artery and necrotic debris with fungal hyphae (Figure 1C). Multiple cranial nerve (II, III, IV, V, VI, VII, IX, X) palsy indicated Garcin syndrome in ROCM with intravenous amphotericin B. She died from multiple organ failure 6 days later.
ROCM, an opportunistic fungal infection of zygomycetes, led to a variety of infections in immunocompromised patients. The angioinvasive characteristics of fungi result in infarction and necrosis of infectious tissues, finally black eschars in the nasal mucosa and palate [1,2]. Biopsy analysis of the necrotic tissue is first recommended for diagnosis of ROCM. CT and MRI are suggested to detect the destruction of periorbital tissues and identify the extent, and vascular thrombosis [1,2]. Total paralysis of all or nearly all unilateral cranial nerves indicates Garcin syndrome. The most causes are primary tumors or metastases of skull base and rhinopharynx, and basal meningitis [1,2]. Infections account for 1% of multiple cranial neuropathies in 979 patients. Three of 50 patients with 8 or more impaired cranial nerves had infections [3]. Early diagnosis of ROCM combined with early intravenous amphotericin B and surgical debridement is recommended to improve the survival rate as well as correction of underlying predisposing factors [1,2].
Declarations
Conflict of interest declaration: None.
Consent: This study was approved by the Institutional Review Board of Taichung Veterans General Hospital (No. CE21215A).
Funding: This work was supported by grants from the Taichung Veterans General Hospital (Grant numbers: TCVGH1107202C). The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- Narayanan S, Panarkandy G, Subramaniam G, Radhakrishnan C, Thulaseedharan NK, Manikath N, et al. The “black evil” affecting patients with diabetes: A case of rhino orbito cerebral mucormycosis causing Garcin syndrome. Infect Drug Resist. 2017; 10: 103-108.
- Yang H, Wang C. Looks like Tuberculous Meningitis, But Not: A Case of Rhinocerebral Mucormycosis with Garcin Syndrome. Front Neurol. 2016; 7: 181.
- Keane JR. Multiple cranial nerve palsies: Analysis of 979 cases. Arch Neurol. 2005; 62: 1714-1717.