
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Hidden in plain site: Papillary thyroid carcinoma with metastases to branchial cleft cyst
Jennifer L Brenner1; Udaya M Kabadi2*
1 Des Moines University, Des Moines, IA, USA.
2 Broadlawns Medical Center, Des Moines University and University of Iowa, Des Moines, IA, USA.
*Corresponding Author: Udaya M Kabadi
Broadlawns Medical Center, 1804 Hickman Road,
Des Moines, Iowa 50314, USA.
Email: oukabadi@gmail.com
Received : Mar 18, 2022
Accepted : Apr 07, 2022
Published : Apr 14, 2022
Archived : www.jcimcr.org
Copyright : © Kabadi UM (2022).
Citation: Brenner JL, Kabadi UM. Hidden in plain site: Papillary thyroid carcinoma with metastases to branchial cleft cyst. J Clin Images Med Case Rep. 2022; 3(4): 1793.
Clinical case
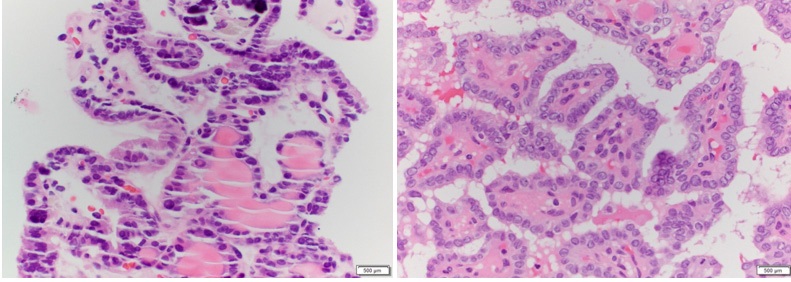
30-year-old female with a history of papillary thyroid carcinoma, status post thyroidectomy and radioactive iodine ablation presented for a routine follow up visit for management of hypothyroidism. Patient was noted to have a congenital branchial cleft cyst in the right superolateral cervical area (Figure 1). Total body scan conducted following ablative I131 dose, 150 mCi had demonstrated no uptake throughout the body including branchial cyst indicative of metastasis. Elevated thyroglobulin tumor marker (14 ng/mL) at this visit was attributed to production by residual thyroid tissue. However, the level continued to rise over the next year to 42 ng/ml. Thyroid ultrasound failed to demonstrate any residual thyroid tissue. Total body scan with I123 scan revealed no uptake anywhere in the body. She also revealed that she has experienced some difficulty swallowing. Repeat thyroid ultrasound noted increase in size of a congenital submandibular branchial cleft cyst with increased vascularity. Therefore, ultrasound guided core needle biopsy of the enlarging right neck mass was performed. Pathology report of the previously known benign branchial cleft cyst showed presence of thyroid epithelium arranged in delicate papillary structures (Figure 2A and 2B). Patient underwent a branchial cyst excision and cervical lymph node dissection.
What is the diagnosis?
Papillary thyroid carcinoma with metastases to branchial cleft cyst
Papillary thyroid carcinoma is the most common thyroid cancer, making up about 80% of all thyroid cancer cases [1]. This is a unique presentation of papillary thyroid carcinoma metastasizing to previously documented benign congenital branchial cleft cyst. Markedly elevated thyroglobulin tumor marker level prompting the biopsy of enlarging branchial cleft cyst became undetectable following excision and has remained undetectable for almost 2 years confirming the branchial cleft cyst as the lone site of metastasis (Figure 1B).
Disclosures: J. L. Brenner: None. U.M. Kabadi: None.


References
- Thyroid Cancer. American Cancer Society. http://www.cancer. org/acs/groups/cid/documents/webcontent/003144-pdf.pdf. Updated January 20, 2012. Accessed March 8, 2012.