
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Two depressed young patients with angina pectoris induced by microvascular dysfunction detected by stress perfusion cardiac magnetic resonance
Jing Wen Yong1#; Jin Fan Tian1#; Jia Xin Cao2; Hui Hui Kong2; Yi He2; Xian Tao Song1*
1 Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, China.
2 Department of Radiology, Beijing Friendship Hospital, Capital Medical University, China.
*Corresponding Author: Xian Tao Song
Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, Chaoyang District,
Anzhen Road NO.2, Beijing city 100029, China.
Email: songxiantao0929@qq.com
Received : Mar 10, 2022
Accepted : Apr 08, 2022
Published : Apr 15, 2022
Archived : www.jcimcr.org
Copyright : © Song XT (2022).
Abstract
Background: Recent evidence indicates a link between depression and microvascular dysfunction, which may affect therapy options and prognosis.
Case summary: We described two young depressed patients with angina. No obstructive coronary heart disease was detected by computed tomography coronary angiography or invasive coronary angiography. Determined by stress perfusion cardiac MRI, these two patients were diagnosed with microvascular angina.
Discussion: The two cases emphasized that depression and microvascular angina can coexist inyoung patients. Negligence of mental disorder may cause insufficient treatments. Both psycho-regulatory interventions and heart disease medicine should be options for these patients.
Keywords: Microvascular angina; Depression; Stress perfusion cardiac magnetic resonance; Case report.
Citation: Yong JW, Tian JF, Cao JX, Kong HH, Song XT, et al. Two depressed young patients with angina pectoris induced by microvascular dysfunction detected by stress perfusion cardiac magnetic resonance. J Clin Images Med Case Rep. 2022; 3(4): 1794.
Introduction
Up to 70% of angina patients who received Invasive Coronary Angiography (ICA) were found to have no obstructive coronary artery stenosis (stenosis degree ≥ 50%) [1], and among them, 26%-54% were with microvascular angina [2].
Clinically, microvascular angina is common, and it is often misdiagnosed as non-cardiac symptoms, leading to inadequate treatments. Especially, microvascular angina patients combined with depression are often neglected and given only psychiatric medication, which may cause them repeatedly seeking medical attention for chest pain symptoms.
Depression is a highly prevalent disease that affects approximately 10% of the population [3]. The prevalence of depression in patients with coronary heart disease is 15-30% [4]. And studies have shown that depression is closely related to peripheral and cerebral microvascular dysfunction [5]. Therefore, it is not surprising that depression is comorbid with microvascular angina. Microvascular angina is closely related to heart failure and myocardial infarction [6]. Moreover, microvascular angina could increase the risk of future cardiovascular events and repeated hospitalizations, reduce the quality of life, and increase medical expenses.
This report describes two depressive patients with angina. Obstructive coronary heart disease was ruled out by Computed Tomography Coronary Angiography (CTA) or Invasive Coronary Angiography (ICA).
They underwent a stress perfusion cardiac MRI, using Adenosine Triphosphate (ATP) as the first-pass vasodilator. We visually compared patients’ stress and rest myocardial perfusion images to determine myocardial ischemia. Circle CVI42 (Circle Cardiovascular Imaging Inc. Canada) was used to evaluate the Myocardial Perfusion Reserve Index (MPRI).
Case series
Case 1
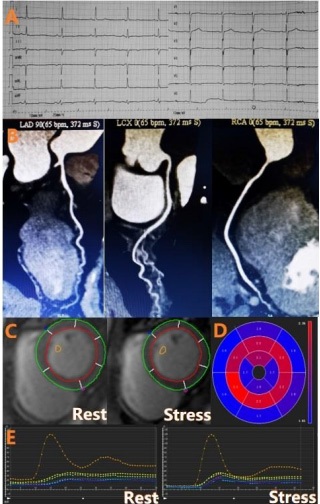
A 32-year-old woman presented to the cardiology clinic due to chest tightness and feeling breathless for 2 months. It mainly occurred during anger and quarrels. Each lasted for 20-30 minutes and was alleviated spontaneously after rest. She couldn’t go to work because of her symptoms. She has been diagnosed with depression for more than two years and has received drugs for depression, including lorazepam, agomelatine and buspirone tablets. She had no history of smoking or drinking. She was not married, having no children. She had menstruation of about 30 days, without, dysmenorrhea.
Her imaging findings were shown in Figure 1 and Table 1. 24-hour Holter showed that 88 there were occasional atrial premature contractions, 642 times every 24 hours, and the dyadic rhythm (64 arrays) was seen; abnormal changes in ST-T (flat T wave in I and V3-V6) were seen in some periods. Echocardiography found she had normal cardiac structure and function, and then her CTCA showed normal coronary artery. She was diagnosed with non-obstructive coronary ischemia.
Table 1: Patients characteristics.
|
Patient 1 |
Patient 2 |
Age/Gender |
32/Female |
36/Male |
ECG |
Flat T wave in I and V3-V6 |
ST-T depression in II and V1-V4 |
CTA/ICA |
Normal |
Normal |
MPRI |
1.51 |
1.93 |
PHQ-9 |
14 |
10 |
GAD-7 |
21 |
9 |
Diagnosis |
Microvascular angina, |
Microvascular angina, |
Management |
Shexiang Tongxin dripping pills, Lorazepam, Agomelatine, Buspirone |
Exercising, Enough sleep |
Follow-up |
6 months |
12 months |
Symptom |
Her symptoms had improved significantly, her seizure frequency was reduced. The patient had not experienced chest discomfort for 1 month. |
The patient had occasional chest discomfort symptoms, 1-2 times a month, mostly when he stayed up late and had high work pressure. |
PHQ-9 |
5 |
8 |
GAD-7 |
5 |
9 |
The myocardial perfusion of adenosine triphosphate in cardiac MRI suggested that there was a ring-shaped area of decreased perfusion under the endocardium of the left ventricle, and the MPRI was abnormal (1.51, normal >2.0). These findings were consistent with the diagnosis of microvascular angina. The cardiologist gave nicorandil (5 mg TID) for treatment. The patient developed headache symptoms after taking nicorandil for 3 days and switched to Shexiang Tongxin dripping pills (2 capsules TID). At 1 month, her symptoms had improved significantly; her symptom frequency was reduced, and she was able to work normally. At 6 months follow-up, the patient had not experienced any chest discomfort for the past 1 month.
Case 2
A 36-year-old man presented to the doctor with a 1-month history of chest pain and chest tightness, mainly in the early morning every day (1-3 times a week), each lasting 3-5 minutes. The symptoms were not related to activities, and most of which occurred during rest. This symptom appeared after the birth of his second child. There was no history of smoking or drinking. He suffered from insomnia because of the great pressure. He was diagnosed with depression for more than 5 years and received medications for depression including fluoxetine and Lorazepam. Two years ago, he stopped medication after the symptoms improved. He had suffered from psoriasis for 12 years and received intermittent medical treatment.
His imaging findings were shown in Figure 2 and Table 1. The Electrocardiogram (ECG) showed abnormal changes of ST-T (STT depression in leads II and V1-V4). The echocardiogram was considered normal, and CTCA also showed normal coronary arteries. His attending cardiologist diagnosed non-obstructive coronary ischemia.
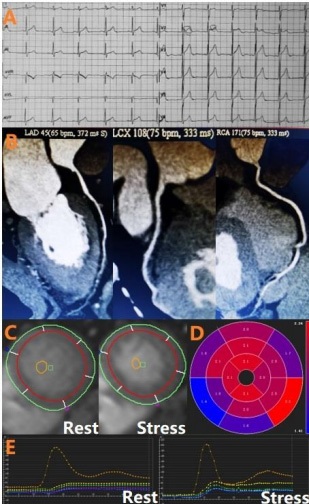
The myocardial perfusion of adenosine triphosphate stress in cardiac MRI suggested that there was a circular area of decreased perfusion under the left ventricular endocardium, and MPRI was abnormal (1.93, normal >2.0). These findings were consistent with the diagnosis of microvascular angina pectoris. Cardiologists treated him with Shexiang Tongxin Dropping Pills (2 capsules TID). At one month, his symptoms had improved significantly, while the frequency of attacks decreased (2 times a month). All drugs were stopped by himself, and his heart symptoms were improved by practicing a healthy lifestyle, including 8 hours of sleep and more than 40 minutes of jogging every day. At 12 months, the patient had occasional chest discomfort symptoms, 1-2 times a month, mostly when he stayed up late and had high work pressure. The frequency of chest pain decreased significantly.
Discussion
Most patients with angina have no obstructive coronary stenosis, notably in women [7,8]. Among these patients, microvascular angina pectoris accounts for a large proportion [9]. Although studies revealed that traditional risk factors (smoking, age, diabetes, hypertension, dyslipidemia, obesity and some proinflammatory indicators) were associated with coronary microcirculatory disturbance [10], the above risk factors could only explain less than 20% of the variation of coronary microvascular dysfunction [11], indicating some other factors contribute to coronary microvascular dysfunction especially among those who are young and without obstructive coronary disease.
We found that some young patients with microvascular angina while without any traditional risk factors often have symptoms of anxiety and depression. Is there a potential link between depression and microvascular angina?
Previous studies have shown that depression is related to brain and peripheral microvascular dysfunction, which may originate from endothelial dysfunction [5]. Moreover, systemic microvascular dysfunction may also lead to the development of depression, and the two promote each other [5].
The underlying mechanism between depression and microvascular angina is not fully understood. Some researchers have suggested that depression leads to unhealthy lifestyles, such as sleep disorders, irregular eating, lack of physical exercise, and smoking [12,13], which are the risk factors for microvascular angina pectoris. In addition, depression increases the risk of diabetes [14], which can cause microvascular angina [15]. Moreover, increased proinflammatory activity and potential immune system disorder may play a role in the link between microvascular angina pectoris and depressive symptoms [16,17].
Recognizing depression symptoms and providing relevant treatment may be a vital and promising strategy to improve the prognosis of young patients with microvascular angina. And it should be practiced in further research and clinical work.
Declarations
Ethics approval and consent to participate: Not applicable.
Consent for publication: A written informed consent form disclosing clinical details and images was obtained from the patient. A copy of the consent form is available for review by the editors of this journal.
Availability of data and material: All relevant data are included in the manuscript.
Competing interests: The authors declare that they have no competing interests.
Funding: This work was supported by Capital Health Development Research Project (No. 2018-2-2063), coronary artery microvascular disease innovation foundation (NO. 2018-CCACMVD-01), National Natural Science Foundation of China (NO. 82100486 and 81971569), and Beijing Municipal Science and Technology Project (Z161100000516139).
Authors’ contributions: JWY drafted the manuscript. JWY and JFT contributed to clinic data collection. JXC and HHK contributed to images collection. XTS made critical revision of the manuscript. YH provided consultation, participated in the design and coordination of the manuscript. All authors read and approved the final manuscript.
Acknowledgements: Thanks for the two patients who participated in this study.
References
- Jacob R, Bachmann TC, Merete H, Sren H, Charlotte S, et al. Prediction of obstructive coronary artery disease and prognosis in patients with suspected stable angina. European Heart Journal 2019; 40: 1426-1435.
- V K, A C, PG C, C B, J E, AHEM M, E P, N K, Y A, C F, et al.An EAPCI Expert Consensus Document on Ischaemia with Non-Obstructive Coronary Arteries in Collaboration with European Society of Cardiology Working Group on Coronary Pathophysiology & Microcirculation Endorsed by Coronary Vasomotor Disorders International Studym Group. European heart journal 2020; 41: 3504-3520.
- Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters E, et al. Prevalence, Severity, and Comorbidity of 12-Month DSM-IV Disorders in the National Comorbidity Survey Replication. JAMA psychiatry. 2005; 62: 590-592.
- Kunadian V, Chieffo A, Camici P, Berry C, Escaned J, et al. An EAPCI Expert Consensus Document on Ischaemia with Non-Obstructive Coronary Arteries in Collaboration with European Society of Cardiology Working Group on Coronary Pathophysiology & Microcirculation Endorsed by Coronary Vasomotor Disorders International Study Group. Eur Heart J. 2020; 41: 3504-3520.
- Patel, Manesh R, Peterson, Eric D, Dai, David, Brennan,et al. Low Diagnostic Yield of Elective Coronary Angiography. New England Journal of Medicine. 2010.
- Jespersen L, Hvelplund A, Abildstr? m, SZ, Pedersen F, Galatius XS, et al. Stable anginapectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. EUROPEAN HEART JOURNAL. 2012.
- Walsh, Mary, Norine, Fleg, Jerome L, et al. Ischemia and No Obstructive Coronary Artery Disease (INOCA) Developing EvidenceBased Therapies and Research Agenda for the Next Decade. Circulation An Official Journal of the American Heart Association 2017.
- Wessel T, Arant C, McGorray S, Sharaf B, Reis S, et al. Coronary microvascular reactivity is only partially predicted by atherosclerosis risk factors or coronary artery disease in women evaluated for suspected ischemia: Results from the NHLBI Women’s Ischemia Syndrome Evaluation (WISE). Clinical cardiology. 2007; 30: 69-74.
- Verger P, Lions C, Ventelou B. Is depression associated with health risk-related behaviour clusters in adults? European journal of public health. 2009; 19: 618-624.
- Katon WJ. Clinical and health services relationships between major depression, depressive symptoms, and general medical illness. Biological Psychiatry. 2003; 54: 216-226.
- Peter R, Jaensch A, Mons U, Schöttker B, Schmucker R, et al. Prognostic value of long-term trajectories of depression for incident diabetes mellitus in patients with stable coronary heart disease. Cardiovascular diabetology. 2021; 20: 108.
- Sara JD, Taher R, Kolluri N, Vella A, Lerman LO, et al. Coronary microvascular dysfunction is associated with poor glycemic control amongst female diabetics with chest pain and non-obstructive coronary artery disease. Cardiovascular Diabetology. 2019; 18.
- CastroאOsta E, Diniz BS, Firmo J, Peixoto SV, Blay SL, et al. Diabetes, depressive symptoms, and mortality risk in old age. The role of inflammation. Depression and anxiety. 2019; 234: 36.
- Alejandro RM, Mason JC, Kaski JC, Rubens MB, Harari OA, et al. Chronic inflammation and coronary microvascular dysfunction in patients without risk factors for coronary artery disease. Euro Heart J. 2009: 1837.