
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Explaining urban-rural disparity in prevalence of stunting and wealth related inequality in Ethiopia: A decomposition analysis
Takele Bekele Hunde
Amhara Regional Agricultural Research Institute, Adet Agricultural Research Center, Bahir Dar, Ethiopia.
*Corresponding Author: Takele Bekele Hunde
Amhara Regional Agricultural Research Institute, Adet
Agricultural Research Center, Bahir Dar, Ethiopia.
Email: bekeletakele@gmail.com
Received : Feb 14, 2022
Accepted : Apr 11, 2022
Published : Apr 18, 2022
Archived : www.jcimcr.org
Copyright : © Hunde TB (2022).
Abstract
Background: Stunting is a global health concern. It has consequences on child survival, growth, and development. The absolute level of stunting has been decreasing in Ethiopia although the prevalence is still high varying across socioeconomic determinants and geographical location with a larger burden among the disadvantaged group and the rural areas. The objective of the study was to explain the rural-urban disparity in the prevalence of stunting and explore the level and determinants of wealth related inequality in stunting in Ethiopia.
Method: Data were drawn from the 2016 Ethiopian Demographic and Health Survey. The dependent variables were stunting and wealth related inequality in stunting. A multivariate decomposition analysis was employed to decompose the urban-rural disparity in the prevalence of stunting into meaningful components. A concentration index was used to quantify the magnitude of inequalities in stunting and multilevel linear regression model was used to identify determinants of socioeconomic inequality in stunting. STATA version 14 software was used for data management and analysis.
Result: Differences in observed characteristics of children, maternal characteristics, their household and environment explained 82.8% of the gap in the prevalence of stunting between rural and urban areas. A further decomposition of the gap in stunting showed that differences in maternal characteristics contributed to 36.7% of the gap in stunting, variation in household characteristics explained 31.7% of the gap and 13.6% of the gap in stunting was due to differences in child characteristics in the two areas. The study also found a significant propoor wealth related absolute inequality in stunting (-0.133). Age of child, maternal education level, maternal age and place of residence were found to be significantly associated with socioeconomic inequality in stunting.
Conclusion: Rural-urban disparities in child stunting need to focus principally on bridging gaps in socio-economic situations of rural and urban women and households and improving the quality of rural infrastructure. Health policy makers should work together across sectors and develop strategies for effective inter sectoral actions to adequately address the social determinants of inequity and reduce inequalities in stunting. Rural-urban disparities in child stunting need to focus principally on bridging gaps in socio-economic situations of rural and urban women and households and improving the quality of rural infrastructure. Health policy makers should work together across sectors and develop strategies for effective inter sectoral actions to adequately address the social determinants of inequity and reduce inequalities in stunting.
Keywords: Ethiopia; Children; Inequality; Disparity; Stunting.
Citation: Hunde TB. Explaining urban-rural disparity in prevalence of stunting and wealth related inequality in Ethiopia: A decomposition analysis. J Clin Images Med Case Rep. 2022; 3(4): 1796.
Background of the Study
Malnutrition is a major health problem in most developing countries. According to the World Health Organization (WHO), malnutrition refers to any disorder of nutrition whether it is due to dietary deficiency or to excess diet which can result from an imbalance between the needs of the body and intake of nutrients. Under nutrition is a general term for a medical condition caused by an insufficient diet. It is any physical condition resulting either from an inappropriate diet or from a physical inability to absorb or metabolize nutrients [35]. Good nutrition allows children to survive, grow, develop, learn, play, participate and contribute, while malnutrition robs children of their futures and leaves young lives hanging in the balance [35].
Child stunting is a public health nutrition problem that hinders the development of future generations, not only physiologically but also potentially deprives their cognitive function and productivity. Stunting represents poor linear growth during a critical period and is diagnosed as a height for age less than -2 standard deviations from the World Health Organization (WHO) child growth standards median (WHO, 2006). Globally, approximately 149 million children under 5 suffer from stunting [36].
Stunted children begin their lives at a marked disadvantage: They face learning difficulties in school, earn less as adults, and face barriers to participation in their communities. More than 90% of the world’s stunted children live in Africa and Asia. More than 37% suffering from stunting are found concentrated in Eastern Africa. Although the prevalence of stunting is decreasing in all regions of the world, Africa is the only region with a rising number of stunted children. In view of this, the absolute number of stunted children in Africa is expected to increase from 56 million in 2010 to 61 million by the year 2025 [36].
The devastating effects of stunting can last a lifetime and even affect the next generation and is strongly associated with numerous short term and long term conditions. These conditions include increased morbidity and mortality, delayed growth, poor children’s well being and social inequalities and long term educational and economic consequences. Thus, the prevention of stunting has been adopted as one of the six main global nutrition targets for the period until 2025 [3]. Despite concrete progress made against child stunting in the past decade Ethiopia remains among countries with the highest number of stunted under five children in the World [9].
The trend, however, shows that the prevalence of stunting has decreased from 58% in 2000 to 37% in 2019, which is an average decline of more than 1% annually, but the problem is still high. Results from the 2019 EMDHS show that 37% of children under 5 are short for their age or stunted, and 12% are severely stunted (below -3 SD). There are some regional variations in stunting, which ranges from a high of 49% in Tigray to a low of 14% in Addis Ababa [7]. This shows that up to the present time, the country has fallen behind expectations with regards to addressing stunting prevalence.
Statements of the problem
Globally, over one third of children in rural households are stunted compared to one quarter in urban households. Child stunting in developing countries have been characterized by large rural-urban disparities over the last few decades [20]. Children in the poorest households are also more likely to be stunted as compared to children in the richest households [4]. In Ethiopia, stunting among children is greater in rural areas (41%) than in urban areas (26%) with 15% differences between urban and rural resident children. Stunting among the poorest and the richest socioeconomic categories was 45.1% and 26.9%, respectively, with an 18% stunting gap between the richest and the poorest socioeconomic categories [7].
Several studies in developing countries have shown that socioeconomic inequality is liked to stunting, such that communities with high socioeconomic inequality carry a disproportionately high burden of stunting [20]. Urban children generally have better nutritional status than rural children, and a number of studies have attempted to explain this difference in stunting between rural and urban children. Differences in the levels of socio-economic characteristics such as maternal education, spouse’s education and the wealth index contribute a major share of rural-urban disparities in child stunting. Differences in the strength of association between socioeconomic characteristics and child stunting account for less than a quarter of rural urban disparities at the lower end of the HAZ score distribution [11,37,12,29,31,28,20,37]. Caregivers education status was the main contributor, accounting alone for (33%) of the socioeconomic inequality in stunting, followed by region of residence (11%) and birth size (6%) [17].
Income inequality between urban and rural households explains most of the stunting gap [24]. Few studies had investigated the urban-rural disparity and related inequality in stunting among under 5 children in Ethiopia [33,31,17,12]. But, the level of the inequality, determinants associated with inequality in stunting and the contribution of the driving factors to the stunting variation, have not yet been enough documented in the case of Ethiopia. Specially, the decomposition of the ruralurban differences based on key socioeconomic variables is not common in case of Ethiopia. Understanding the nature and the causes of this urban-rural and wealth related inequality is essential in planning child health and improving the gap in child health outcome in urban and rural areas. The present study, therefore attempts to investigate the contribution of different factors to the urban-rural gap in stunting and identify the determinants of stunting inequality in Ethiopia.
The general objective of the study was to decompose the rural-urban disparity in the prevalence of stunting and to explore the level and determinants of inequality in stunting in Ethiopia.
The specific objectives of the study which should be accomplished to achieve the general objective stated above are:
• Decompose rural-urban disparity in stunting, • Explore the level of inequality in stunting, and • Identify determinants of inequality in stunting this research tries to answer the following questions: • What is the level of inequality in stunting in Ethiopia? • What explains the inequality in stunting in Ethiopia? • What contributes to the urban- rural gap in stunting in Ethiopia?
Methods and materials
Population and data source
The data for this study was obtained from Ethiopia Demography and Health Surveys (EDHSs) conducted in 2016. The 2016 Ethiopia Demographic and Health Survey (EDHS) were implemented by the Central Statistical Agency (CSA). By virtue of its mandate, the CSA has conducted the surveys in collaboration with the Federal Ministry of Health (FMoH) and the Ethiopian Public Health Institute (EPHI) with technical assistance from ICF international, and financial as well as technical support from development partners. The 2016 survey was conducted from January 18, 2016, to June 27, 2016, based on a nationally representative sample. The 2016 Ethiopian Demographic and Health Surveys, were designed to provide estimates for the health and demographic variables of interest for the following domains: Ethiopia as a whole; urban and rural areas (each as a separate domain); and 11 geographic administrative regions (nine regions namely: Tigray, Affar, Amhara, Oromiya, Somali, Benishangul Gumuz, Southern Nations, Nationalities and Peoples, Gambela and Harari regional states and two city administrations : (Addis Ababa and Dire Dawa) [6]. DHS surveys are one of the most cited databases globally and have been conducted in over 90 countries since 1984 [6]. All children included in the survey were below 5 years of age.
Description of the variables in the study
The response variable: The dependent variables were modeled in two different ways. Firstly, the study used stunting as a binary variable that indicated whether or not the child was stunted (i.e., two standard deviations or more below the mean of the WHO reference population). Secondly, the study used HAZ scores in their continuous form to model the determinants for socioeconomic inequalities in stunting that is wealth related inequality in Stunting as dependent variable. Stunting, or linear growth failure, is defined when HFA is below -2 Z-scores [36]. The study used height-for-age z-scores to measure the contribution of each determinant to the urban-rural disparity in stunting and concentration index to indentify determinants of inequality in stunting [38].
Explanatory variables: The explanatory variables included in this study are based on the related literature including report on the causes and consequences of stunted growth published by WHO (2017) and the widely applied UNICEF framework (UNICEF 1992) outlining the causes of stunting with some modification and also these determinants of child stunting were obtained from the available similar studies reviewed above and available data on the subject. The study used children’s characteristics (age of child in months, sex of child, birth order number and size of child at birth) maternal characteristics (place of delivery, partner’s/husband education level, age at first birth, maternal education status, Religion of mother’s, maternal working status and body mass index) and household characteristics (sex of household head, region of residence and wealth index) as determinants factors. Postnatal care service utilization and ANC are excluded in the entire analysis due to the missing value.
Methods of data analysis
All analyses were done taking into account the complex design of the survey. Thus, all estimates reported were based on the weighted sample (n= 9588), not on the unweighted sample (n=8855). The weighting was done to adjust for the inequality in sampling probability due to the over representation of small states (region) [6]. All analysis was conducted using STATA 14 software, with statistical significance determined at ≤0.05. The analysis starts with an analysis of the individual variables separately. The purpose of this was to examine the proportion of respondents with specific characteristics including the dependent variable, child stunting. Bivariate analysis was done to determine the relationship between the socioeconomic variables and urban-rural disparity in stunting. Socioeconomic inequality was measured using an alternative concentration index that avoids problems with dependence on the mean level of stunting [20].
Concentration index is a relative measure of inequality that indicates the extent to which stunting is concentrated among the disadvantaged or the advantaged. The gap in stunting between the urban and rural groups was decomposed into its contributing determinants, following the Blinder Oaxaca decomposition approach, specifically the multivariate decomposition for linear regression models. A Blinder- Oaxaca decomposition analysis will be conducted to decompose the rural-urban differences in stunting into two components; one that is explained by differences in the level of the determinants (covariate effects), another component that is explained by differences in the effect of the determinants on the child stunting status (coefficient effects). The decomposition method developed by Blinder (1973) and Oaxaca (1973), and generalized by Neumark (1988) and Oaxaca and Ransom (1988,1994), allows the decomposition of outcome variables between two groups into a part that is explained by differences in observed characteristics and a part attributable to differences in the estimated coefficients [27].
Econometric analysis
The econometric analysis was performed at three levels; first concentration curves for the child stunting variables were constructed. Second, the concentration indices for these variables were computed to augment the concentration curves. The final analysis was done to identify the determinants of the inequality in stunting and to identify factors that contribute to wealth related inequality in child stunting.
The concentration curve gives a pictorial view of the pattern and magnitude of inequality in child stunting. The curve is a plot of the cumulative percentage of child stunting on the y-axis and wealth status ranked by cumulative percentage of the population on the X-axis.
The concentration curves depict inequality against the poor if it lies above the line of equality (450 line). On the other hand, inequality against the rich exists if the curve lies below the line of equality. In a situation where there exists perfect equality in child stunting, irrespective of wealth status, the concentration curve is a straight line equal to the 450 line. The magnitude of inequality is depicted by how far the curve lies away from the line of equality. For instance, if the magnitude of inequality in favour of the rich is higher, the farther the curve will be above the line of equality. To ascertain the magnitude and nature of wealth related inequality in child stunting, the Concentration Indices (CI) were computed. This approach of measuring inequality has been widely used and recognized as a standard tool. The Concentration index summarizes the information contained in each concentration curves and is twice the area between concentration curves and equity line [38].
Concentration indexes were calculated to measure the gap between the concentration curves and the equity line. If the curves lie below the equity line, stunting would be more concentrated among people in the upper socioeconomic strata, and the value of concentration indices would be positive. Moreover, a value of 0 (zero) signifies perfect equality, i.e., there is no socioeconomic related inequity for child stunting.
The relationship between the factors and the wealth related inequality in stunting was done to identify the determinants of inequality in stunting by using multilevel linear regression models using the stata command regress.
Three different models were fit: Model 1 was fit for child and maternal characteristics, model 2 for context variables, and model 3 is the final model fit only for variables that have shown association with the inequality at 20% level of significance.
Where Yijk indicates that level of wealth related inequality in stunting of child i in a household j and community k, X1 vectors of child and maternal characteristics and X2 is context variables. While β is a vector of regression coefficients and γo and γ1 are mean zero random variables.
Multivariate decomposition
A multivariate decomposition (Blinder–Oaxaca decomposition) analysis was used to decompose the urban-rural disparity in stunting. The decomposition technique separates the contribution of characteristics of respondents and their environment as well as characteristics of children, endowment effect, in one hand and the contribution of response to behavior, coefficient effect, on the other. The Blinder–Oaxaca decomposition is a statistical method that explains the difference in the means of a dependent variable between two groups by decomposing the gap into a part is due to differences in the mean values of the independent variable within the groups, on the one hand, and group differences in the effects of the independent variable, on the other hand [34]. The methodology employed in this study allows us to decompose rural-urban differences in child stunting into covariate and coefficients effect further enables us to quantify the contribution of individual explanatory variables to rural-urban differences via these effects. This technique decomposes the gap in stunting between urban and rural into two parts; a part that is due to difference in the distribution of the determinants of stunting (covariates effect) between urban and rural and due to the difference in the effect of these determinants (coefficients effect) between urban and rural [34].
For example, if yi, our outcome variable, is affected by a single variable, x, and we have two groups, urban and rural, then stunting for the rural and urban children are given by Eqs. (1) and (2) respectively
Yurban =βurban xi +εurban if a child belongs to an urban household (1)
Yrural =βrural xi +εrural if a child belongs to rural household (2)
Thus the urban-rural gap in the mean stunting (Yurban - Yrural) is given as in Eq.(3)
Yurban - Yrural =βurbanxurban – βruralxrural (3)
Where xurban and xrural are the explanatory variable at their means for the urban and rural. The overall urban rural gap could be decomposed into a gap that is attributable to difference in the level of the covariates, X’s, and a gap that is attributable to difference in coefficients, β ‘ s as in Eqs. (4) and (5):
Where the overall urban-rural gap in child stunting is comprised of the gap in endowment (E) and the gap between coefficients (C). First the index of the dependent variable was produced using the rifireg stata command using wealth index as a ranking variable. Then decomposition can be done by using the stata command oaxaca_rif and normalize Child stunting characteristic in to three groups (child related characteristics, maternal related characteristics and context variables).
Results
Background characteristics
A total of 9588 weighted cases of under five children were utilized for the present analysis, 1048 from urban and 8540 from rural areas of Ethiopia. More than half, 54.2% in urban and 58.6% in rural areas were children of at least 24 months of age. The proportion of male children in both urban and rural areas were a little higher than female children and a quarter of the births were small sized at birth (25.9%), 19.2% in urban and 26.8% in rural. While births of higher order (6 or more) are common in rural areas (29.1% in rural versus 9.9% in urban), first births are more common in urban than rural areas (31.8% against 16.6%).Similarly, births of order 2-3 are more prevalent in urban areas (42.5%) than rural areas (29.4%); but, birth orders of 4-5 are more prevalent in rural areas (24.9%) than urban areas (15.9). The majority of urban children (79.9%) were born in a health facility whereas 78.3% of the rural children were delivered at home.
The proportion of estimated size of children at birth in rural areas for about a quarter of them was smaller sizes (26.8%) in urban areas the proportion was one in five (19.2%) (Table 1).
Table 1: Percent distribution of child related characteristics by place of residence, EDHS 2016.
Variables and categories |
Place of residence |
||
Urban (n=1048) |
Rural (n=8540) |
Total (n=9588) |
|
Child age in months |
|
|
|
<6 |
12.02 |
11.23 |
11.32 |
6-11 |
13.05 |
10.41 |
10.7 |
12-23 |
20.74 |
19.78 |
19.88 |
24-59 |
54.19 |
58.58 |
58.1 |
Child's sex |
|
|
|
Male |
51.88 |
50.93 |
51.03 |
Female |
48.12 |
49.07 |
48.97 |
Size of baby at birth |
|
|
|
Otherwise |
80.85 |
73.23 |
74.06 |
Small |
19.15 |
26.77 |
25.94 |
Birth order |
|
|
|
First |
31.77 |
16.63 |
18.29 |
2-3 |
42.47 |
29.38 |
30.81 |
4-5 |
15.86 |
24.89 |
23.9 |
6 and above |
9.90 |
29.09 |
26.99 |
Place of delivery |
|
|
|
Home |
20.06 |
78.33 |
71.96 |
Health Facility |
79.94 |
21.67 |
28.04 |
Maternal characteristics are also summarized and the result is shown in the table below. A total of 6972 mothers, 869 in urban and 6103 in rural areas, were included in the analysis.
Teenage mothers prevailed in rural areas with a very high magnitude (66.4%) than urban areas (45.0%). In rural areas, more than two-third (68.9%) of the mothers had no formal schooling and mothers having a secondary and above level of education were very limited (3.5%). Contrarily, in urban areas, a quarter of the mothers had no formal schooling (24.0%) and two in five of them had an above primary level of educational achievement (42.6%). Three quarter of the women in rural areas (74.7%) were not engaged in paid work whereas about half of the women of urban areas (48.1%) were working at the time of the survey (Table 2).
Table 2: Percent distribution of maternal characteristics by place of residence, EDHS 2016.
Variables and categories |
Place of residence |
||
Urban (n=869) |
Rural (n=6103) |
Total (n=6972) |
|
Age at first birth |
|
|
|
20+ |
55.05 |
33.6 |
36.27 |
<20 |
44.95 |
66.4 |
63.73 |
Maternal education |
|
|
|
No education |
24 |
68.88 |
63.29 |
Primary |
33.46 |
27.63 |
28.35 |
Secondary+ |
42.55 |
3.49 |
8.36 |
Current age of mother |
|
|
|
15-24 |
18.67 |
24.23 |
23.53 |
25-34 |
62.91 |
49.42 |
51.1 |
35+ |
18.42 |
26.35 |
25.36 |
Current work status |
|
|
|
No |
51.88 |
74.69 |
71.85 |
Yes |
48.12 |
25.31 |
28.15 |
Religion |
|
|
|
Christian |
76.61 |
58.31 |
60.59 |
Muslim |
23.04 |
39.38 |
37.34 |
Others |
0.34 |
2.31 |
2.06 |
BMI of Mothers* |
n=859 |
n=6043 |
n=6901 |
Underweight |
10.1 |
21.14 |
19.77 |
Normal |
63.49 |
74.97 |
73.54 |
Overweight |
19.81 |
3.42 |
5.46 |
Obese |
6.60 |
0.47 |
1.23 |
Partner’s education* |
n=785 |
n=5722 |
n=6507 |
No education |
16.96 |
51.06 |
46.94 |
Primary |
30.26 |
40.59 |
39.35 |
Secondary |
25.90 |
6.30 |
8.67 |
Tertiary |
26.88 |
2.05 |
5.05 |
* These characteristics have missing observations
In urban areas, the proportions of mothers of age 25-34 were 62.9% having a wider percentage point difference with that of rural area (49.4%). Again, in urban areas the share of Christian religion was 76.6% and about a quarter of the mothers (23.0%) were Muslim. The share of Muslim religion was much higher in rural area (39.4%) and shrank the share of Christian religion (58.3%) than the urban counterpart. As for partner’s education, more than half (52.8%) of the partners of urban women had an above primary level of education while 51.1% of partners of women of rural areas had no formal schooling. Underweight was common among rural women (21.1%) than urban women (10.1%). Contrarily, overweight and obesity was a characteristic of urban women (19.8% overweight and 6.6% obese) than rural women (3.4% and 0.5%) (Table 2 & Table 3).
Table 3: Percent distribution of household characteristics by place of residence, EDHS 2016.
Variables and categories |
Place of residence |
||
Urban (n=857) |
Rural (n=6022) |
Total (n=6879) |
|
Sex of the household head |
|
|
|
Female |
25.44 |
12.5 |
14.12 |
Male |
74.56 |
87.5 |
85.88 |
Region |
|
|
|
Tigray |
10.66 |
6.69 |
7.19 |
Afar |
1.29 |
0.8 |
0.86 |
Amhara |
23.42 |
21.75 |
21.96 |
Oromia |
21.28 |
43.77 |
40.97 |
Somali |
4.28 |
3.27 |
3.39 |
Benishangul Gumuz |
0.68 |
1.09 |
1.04 |
SNNPR |
15.19 |
22.08 |
21.22 |
Gambela |
0.83 |
0.17 |
0.25 |
Harari |
0.64 |
0.15 |
0.21 |
Addis Ababa |
20.17 |
NA |
2.51 |
Dire Dawa |
1.57 |
0.23 |
0.39 |
Household wealth |
|
|
|
Poorest |
22.02 |
20.58 |
20.76 |
Poor |
19.77 |
22.03 |
21.75 |
Middle |
23.48 |
20.71 |
21.06 |
Richer |
19.76 |
19.02 |
19.11 |
Richest |
14.97 |
17.66 |
17.32 |
NA= Not Applicable
A total of 6879 households were interviewed for the under five children survey, 857 in urban and 6022 in rural areas. A quarter of the households in urban areas were female headed (25.4%) and 12.5% of the rural households were headed by women. An almost equal proportion of households were interviewed in the each of the wealth categories by residence.
The largest urban household shares were from Amhara (23.4%), Oromia (21.3%) and SNNP (15.2%) and Addis Ababa (20.2%). On the other hand, Oromia contributed the largest share of households in the rural area (43.8%) followed by SNNP (22.1%) and Amhara (21.8%) (Table 3).
Differentials of stunting
Prevalence of stunting across selected child characteristics by place of residence is shown in the table below. The prevalence of stunting showed a progressive increase across the age of the child in both areas. Sex of the baby did not show differences on stunting in both urban and rural areas, that is, a significant difference was not observed between the sexes within the two residences. Small size births in urban areas exhibited a higher rate of stunting (33.4%) than otherwise (21.8%). In rural areas, though the magnitude of stunting is higher than urban areas, the risk difference in stunting between small sized births (43.9%) and non-small sized births (37.3%) is very small. The prevalence of stunting among home delivered babies in both areas is nearly the same, 37.0% in urban and 40.5% in rural. However, health facility delivery had a differential impact on stunting in urban areas (20.7%) and rural areas (34.8%). The analysis also revealed that birth order had no observable influence over stunting in rural areas; but, in urban areas, higher birth ordered children were highly affected by stunting as shown by the jump in the prevalence from around 20% for smaller birth orders to 30% among higher ordered births (Table 4).
Table 4: Prevalence of stunting by child characteristics disaggregated by place of residence, EDHS 2016.
Characteristics and categories |
Residence |
|
Urban (n=1048) |
Rural (n=8540) |
|
Child age in months |
||
<6 |
0.079 |
0.141 |
11-Jun |
0.092 |
0.171 |
23-Dec |
0.268 |
0.413 |
24-59 |
0.293 |
0.470 |
Child's sex |
|
|
Male |
0.259 |
0.407 |
Female |
0.220 |
0.376 |
Size of baby at birth |
|
|
Otherwise |
0.218 |
0.373 |
Small |
0.334 |
0.439 |
Birth order |
|
|
First |
0.225 |
0.378 |
2-3 |
0.206 |
0.382 |
4-5 |
0.311 |
0.404 |
6+ |
0.319 |
0.400 |
Place of delivery |
|
|
At Home |
0.370 |
0.405 |
Health Facility |
0.207 |
0.348 |
Prevalence |
0.260 |
0.410 |
Children born to teenage mothers have a tendency of being stunted. The contrast in prevalence of stunting between teenage mothers and non-teenage mothers in urban areas is higher (27.1% versus 21.6%) as opposed to their rural counterparts (40.1% versus 37.4%). Maternal education greatly benefited their children in that the likelihood of being stunted reduces with the level of maternal education in both areas. Partner’s education has also shown a positive influence on the likelihood of stunting as shown in the progressive decline of the rate of stunting with the increase in the level of education. Underweight mothers have a tendency of bearing stunted children while overweight and obese mothers have a reduced likelihood of having a stunted child (Table 5).
Table 5: Prevalence of stunting by maternal characteristics disaggregated by place of residence.
Variables and categories |
Residence |
|
Urban (n=1048) |
Rural (n=8540) |
|
Age at first birth |
|
|
20+ |
0.216 |
0.374 |
<20 |
0.271 |
0.401 |
Maternal education |
|
|
No education |
0.330 |
0.410 |
Primary |
0.252 |
0.364 |
Secondary+ |
0.162 |
0.253 |
Current age of mother |
|
|
15-24 |
0.256 |
0.362 |
25-34 |
0.228 |
0.394 |
35+ |
0.255 |
0.418 |
Current work status |
|
|
No |
0.239 |
0.384 |
Yes |
0.241 |
0.416 |
Religion |
|
|
Christian |
0.216 |
0.391 |
Muslim |
0.274 |
0.391 |
Others |
0.375 |
0.445 |
BMI of Mothers* |
|
|
Underweight |
0.364 |
0.413 |
Normal |
0.260 |
0.389 |
Overweight |
0.145 |
0.309 |
Obese |
0.148 |
0.250 |
Partner’s education* |
|
|
No education |
0.361 |
0.418 |
Primary |
0.263 |
0.369 |
Secondary |
0.213 |
0.334 |
Tertiary |
0.144 |
0.283 |
Prevalence |
0.260 |
0.410 |
Sex of the household head does not seem to have a sizeable influence over the likelihood of stunting in both residences. The progressive decline in the prevalence of stunting with an advance in household wealth in both urban and rural areas is an indication of the presence of inequality in stunting in both areas. In Somali region, the prevalence of stunting is nearly the same over residences (25.5% in urban and 27.7% in rural). In Dire Dawa, the magnitude in rural areas is nearly double as compared to the level in urban area (51.5% versus 25.9%). In urban areas, the magnitude of stunting is the highest in urban areas of Amhara region (38.3%) and the least in urban Oromia (11.5%). In rural areas, the least prevalence is observed in Somali region and the maximum in Dire Dawa (Table 6).
Table 6: Prevalence of stunting by household characteristics disaggregated by place of residence, EDHS 2016.
Variables and categories |
Residence |
|
Urban (n=1048) |
Rural (n=8540) |
|
Sex of the household head |
|
|
Female |
0.256 |
0.383 |
Male |
0.233 |
0.394 |
Region |
|
|
Tigray |
0.338 |
0.409 |
Afar |
0.360 |
0.446 |
Amhara |
0.383 |
0.476 |
Oromia |
0.115 |
0.371 |
Somali |
0.255 |
0.277 |
Benishangul Gumuz |
0.333 |
0.447 |
SNNPR |
0.329 |
0.39 |
Gambela |
0.203 |
0.28 |
Harari |
0.215 |
0.365 |
Addis Ababa |
0.146 |
NA |
Dire Dawa |
0.259 |
0.515 |
Household wealth |
|
|
Poorest |
0.456 |
0.406 |
Poor |
0.342 |
0.436 |
Middle |
0.316 |
0.375 |
Richer |
0.312 |
0.337 |
Richest |
0.217 |
0.297 |
Prevalence |
0.260 |
0.410 |
NA= Not Applicable
Determinants of inequality in stunting
The determinants of wealth related inequality in stunting were identified using a multilevel linear regression model. Three different models were fit: model 1 was fit for child and maternal characteristics, model 2 for context variables, and model 3 is the final model fit only for variables that have shown association with the inequality at 20% level of significance. The result is displayed in the table shown under (Table 7).
Table 7: Multivariate decomposition analysis result for gap in prevalence of stunting between rural and urban children, EDHS 2016.
Contribution |
Value |
P-Value |
[95%conf.Interval] |
% |
|
LL |
UL |
||||
Endowment |
11.3 |
0.000 |
5.5 |
17.1 |
82.8 |
Coefficient |
2.4 |
0.500 |
-4.5 |
9.2 |
17.2 |
Difference in prevalence of |
13.7 |
0.000 |
9.9 |
17.5 |
100.0 |
CI: Confidence Interval; LL: Lower Limit; UL: Upper Limit.
After controlling the influence of level one characteristics, the pro-poor inequality was found to be wider in among urban children (β=-0.164) as opposed to rural children. The propoor inequality in stunting is higher among older infants (6-11 months) and children of age above 1 year as opposed to young infants g infants (<6 month) as evidenced by the negative significant coefficient (Model 3-Table 7).
The pro-poor wealth related inequality in stunting is visibly seen among children born to older women than younger mothers (β=-0.101). Moreover, children born to educated women (secondary and above) were severely affected by the inequality in stunting than children of uneducated women (β=-0.221). It has also been confirmed that maternal education also played a role in widening the gap in prevalence of stunting between urban and rural areas (Table 8 & Model 3-Table 7).
Table 8: Detailed multivariate decomposition of stunting-endowment Effect, EDHS 2016.
Variables and categories |
Coef. |
P-Value |
95% CI |
% |
|
LL |
UL |
||||
Child related characteristics |
|
|
|
|
13.6 |
Child age (in months) |
|
|
|
|
7.9 |
<6 |
0.076 |
0.000 |
0.053 |
0.099 |
0.555 |
11-Jun |
0.434 |
0.000 |
0.294 |
0.574 |
3.171 |
23-Dec |
-0.155 |
0.000 |
-0.194 |
-0.116 |
-1.133 |
24-59 |
0.727 |
0.000 |
0.611 |
0.843 |
5.316 |
Birth order |
|
|
|
|
3.7 |
First |
0.219 |
0.495 |
-0.409 |
0.846 |
1.597 |
2-3 |
-0.007 |
0.966 |
-0.338 |
0.32396 |
-0.0529 |
4-5 |
-0.024 |
0.844 |
-0.262 |
0.214 |
-0.175 |
6+ |
0.322 |
0.349 |
-0.352 |
0.995 |
2.351 |
Female children |
-0.055 |
0.003 |
-0.091 |
-0.019 |
-0.402 |
Small size births |
0.536 |
0.000 |
0.320 |
0.752 |
3.918 |
Facility delivery |
-0.216 |
0.841 |
-2.324 |
1.892 |
-1.578 |
Maternal characteristics |
|
|
|
|
36.7 |
Age at first birth |
0.041 |
0.906 |
-0.647 |
0.729 |
0.302 |
Maternal education |
|
|
|
|
26.7 |
None |
1.535 |
0.066 |
-0.104 |
3.173 |
11.218 |
Primary |
-0.191 |
0.140 |
-0.444 |
0.062 |
-1.395 |
Secondary+ |
2.305 |
0.055 |
-0.046 |
4.657 |
16.855 |
Maternal age |
|
|
|
|
1.0 |
15-24 |
0.148 |
0.086 |
-0.021 |
0.316 |
1.079 |
25-34 |
0.118 |
0.326 |
-0.117 |
0.352 |
0.859 |
35+ |
-0.132 |
0.212 |
-0.339 |
0.075 |
-0.964 |
Religion of the mother |
|
|
|
|
-4.7 |
Christian |
0.110 |
0.795 |
-0.722 |
0.943 |
0.808 |
Muslim |
-0.853 |
0.027 |
-1.608 |
-0.098 |
-6.237 |
Others |
0.102 |
0.174 |
-0.045 |
0.248 |
0.743 |
BMI of the mother |
|
|
|
|
6.3 |
Underweight |
0.120 |
0.721 |
-0.539 |
0.780 |
0.880 |
Normal |
0.074 |
0.781 |
-0.451 |
0.600 |
0.544 |
Overweight |
0.901 |
0.124 |
-0.247 |
2.049 |
6.588 |
Obese |
-0.233 |
0.607 |
-1.124 |
0.657 |
-1.707 |
Partner’s education |
|
|
|
|
7.1 |
None |
0.711 |
0.224 |
-0.435 |
1.858 |
5.2 |
Primary |
-0.117 |
0.532 |
-0.484 |
0.250 |
-0.856 |
Secondary |
-0.374 |
0.435 |
-1.314 |
0.565 |
-2.736 |
Tertiary |
0.756 |
0.440 |
-1.162 |
2.674 |
5.529 |
Context variables |
|
|
|
|
31.9 |
Household wealth |
|
|
|
|
31.9 |
Poorest |
0.624 |
0.023 |
0.087 |
1.160 |
4.559 |
Poor |
0.913 |
0.007 |
0.249 |
1.578 |
6.678 |
Middle |
-0.063 |
0.839 |
-0.665 |
0.540 |
-0.458 |
Richer |
-0.395 |
0.094 |
-0.857 |
0.067 |
-2.885 |
Richest |
3.280 |
0.118 |
-0.834 |
7.395 |
23.981 |
CI: Confidence Interval; LL: Lower Limit; UL: Upper Limit.
The Intra Class Correlation (ICC) report (Table 8) one intra class correlation for this three- level mixed model. The level on first model intra class correlation, correlation between child characteristics and maternal characteristics. There is no a strong correlation between child characteristics and maternal characteristics included in the model.
Inequality in stunting
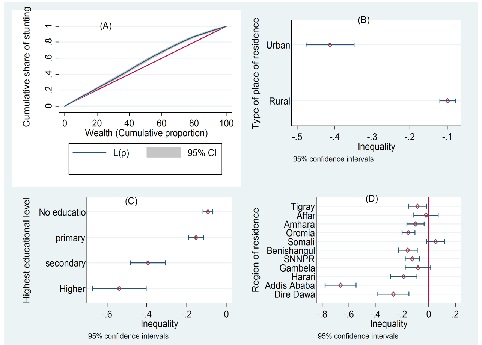
As is shown in the graph below (Panel A), the absolute inequality in stunting is a negative quantity indicating a pro-poor inequality. That is child stunting is more concentrated among the poor socioeconomic groups. The wealth related inequality in stunting is the worst among births to mothers having a secondary and above level of education (Panel C). In addition, analysis of inequality showed that the gap in the level of stunting between affluent households and the poor is much wider in urban areas than rural households (Panel B). Addis Ababa is hard hit by the wealth related absolute inequality in stunting. However, the inequality is absent in three regions, that is, Afar, Somali, and Gambela (Panel D) (Figure 1).
Decomposition analysis
The urban rural gap in the prevalence of stunting (13.7%) is decomposed into endowment and coefficient effects. The result of the decomposition analysis is displayed in the table below. The multivariate decomposition analysis revealed that a significant proportion of the gap in stunting (11.3%) is explained by compositional effects (82.8%). Differential effects of characteristics in urban and rural areas accounted 17.2%, that is, a 2.4 percentage point difference. As the decomposition result for the coefficient effects is not significant, only the result for endowment effects are displayed (Table 9).
Table 9: Multilevel linear regression model for wealth related inequality in stunting, EDHS 2016.
Variables and categories |
Model 1 |
Model 2 |
Model 3 |
|||||
Coef. |
P-value |
Coef. |
P- |
Coef. |
St.Err. |
P-value |
Sig |
|
Child age (<6 [ref]) |
|
|
|
|
|
|
|
|
6-11 |
-0.155 |
0.001 |
|
|
-0.149 |
0.043 |
0.001 |
*** |
12-23 |
-0.171 |
0.000 |
|
|
-0.17 |
0.045 |
0.000 |
*** |
24-59 |
-0.165 |
0.000 |
|
|
-0.17 |
0.043 |
0.000 |
*** |
Female child |
0.019 |
0.402 |
|
|
|
|
|
|
Birth order (1st [ref]) |
|
|
|
|
|
|
|
|
2-3 |
0.013 |
0.718 |
|
|
-0.001 |
0.035 |
0.987 |
|
4-5 |
0.101 |
0.025 |
|
|
0.066 |
0.045 |
0.143 |
|
6+ |
0.108 |
0.025 |
|
|
0.058 |
0.048 |
0.228 |
|
Maternal education |
|
|
|
|
|
|
|
|
Primary |
-0.079 |
0.01 |
|
|
-0.04 |
0.031 |
0.191 |
|
Secondary + |
-0.34 |
0.000 |
|
|
-0.221 |
0.055 |
0.000 |
*** |
Religion of the mother |
0.000 |
|
|
|
|
|
|
|
Muslim |
-0.007 |
0.822 |
|
|
|
|
|
|
Others |
-0.02 |
0.852 |
|
|
|
|
|
|
Working mother |
-0.029 |
0.283 |
|
|
|
|
|
|
Maternal age (15-24 ref]) |
|
|
|
|
|
|
|
|
25-34 |
-0.094 |
0.008 |
|
|
-0.057 |
0.035 |
0.11 |
|
35+ |
-0.156 |
0.001 |
|
|
-0.101 |
0.05 |
0.042 |
** |
Urban |
|
|
-0.169 |
0.019 |
-0.164 |
0.072 |
0.022 |
** |
Women education |
|
|
-0.269 |
0.064 |
-0.036 |
0.149 |
0.809 |
|
Well-off households |
|
|
-0.127 |
0.104 |
-0.111 |
0.078 |
0.158 |
|
According to the detailed decomposition displayed in the table below, compositional differences in child and maternal characteristics accounted for 13.6% and 36.7% of the gap in the prevalence of stunting between rural and urban children, respectively. Differences in educational achievement of rural and urban women was the prime maternal related characteristics that contributed to 26.7% of the gap in stunting. Trailing behind maternal education, differences in partner’s education (7.1%) and BMI of mothers (6.3%) also contributed to the gap in prevalence of stunting the two areas. Child age composition (7.9%) and differences in the birth order of urban rural children (3.7%) are the child related characteristics that would result in the reduction of the gap in the prevalence of stunting in the two residences.
Contrarily, if the religious composition of women of rural area were to be similar to that of women of urban area, the gap in prevalence of stunting would increase benefiting rural children (note the percent contribution to the gap is -4.7%). Similarly, facility delivery, however small the contribution (-1.6%), would widen the gap in stunting. On the other hand, the analysis suggested that equalizing the wealth distribution of rural households to that of urban households alone would be expected to reduce the rural-urban gap in the prevalence of stunting by about 32%. Generally, it has been observed that it is not only child and maternal characteristics but also context variables contributed to the gap in the prevalence of stunting in the two areas.
Table 10:
Level |
ICC |
Std.Err. |
[95% Conf.Interval] |
|
Clusters |
0.048 |
0.026 |
0.017 |
0.132 |
Discussion
The study demonstrated explaining urban-rural disparity in prevalence of stunting and wealth related inequality among children under 5 years of age in Ethiopia based on nationally representative data of the year 2016. Consequently, Descriptive statistics, concentration index, multilevel linear regression model and multivariate decomposition data analyses were employed. The results of the study shows that rural households have lower access to place of delivery than urban households and child born in rural household have lower size at birth than urban children. Rural mothers are less educated, less an employed, have lower access to satisfactory sanitation and improved drinking water than urban households. This is also supported by several studies that have reported large urban and rural differences in socioeconomic conditions [24,30]. The results of the study also show that in rural areas there are very high magnitudes of teenagers mothers than urban areas. The study shows that underweight was common among rural women than urban. Nearly half of the rural households were in the poorest and poorer wealth quintiles.
This study found that age of the child significantly affected the child’s stunting status that is risk of stunting increased along with increase in the age of a child in both areas. Recent studies were reported similar finding in Bangladesh [18], Madagascar [22] and Malawi [19].
It could be due to the inappropriate and late introduction of low nutritional quality supplementary food [5], and a large portion of guardian in rural areas are ignoring to meet their children’s optimal food requirements as the age of the child increases [8].
It could be due to the inappropriate and late introduction of low nutritional quality supplementary food [5], and a large portion of guardian in rural areas are ignoring to meet their children’s optimal food requirements as the age of the child increases [8]. It could be due to the inappropriate and late introduction of low nutritional quality supplementary food [5], and a large portion of guardian in rural areas are ignoring to meet their children’s optimal food requirements as the age of the child increases [8].
Health facility delivery had a differential impact on stunting in urban and rural. The study found increased risk of stunting in children under 5 years of teenage mothers suggesting an increased risk of child stunting with young maternal age in both urban and rural areas. Child born from teenage mothers are more likely to be of low birth weight with the risk of associated long term effects. Children of teenage mothers compared to those of adult mothers were at least three times more likely to be stunted [39]. This study identified Maternal education greatly benefited their children in that the likelihood of being stunted reduces with the level of maternal education in both areas. The child stunting was found to be inversely related to the mother’s level of education. Compared with a child with higher maternal education, a child with lower maternal education has more risk of being in a worse stunting. Children whose mothers have higher education were less likely to be stunted as compared with children whose mother had lower or no education. As educated mothers have better knowledge of child health and nutrition, they are more conscious of their child’s health and look after their children better. This is supported with reports of previous finding from Ethiopia [17,8], India [26] and Sirlanka [14].
This finding shows the importance of the education of girls as alternative strategy to beat the burden of child stunting. Not only maternal education but also father’s education has significant impact on child stunting, and children whose father attended formal education had less chance of being stunting in both urban and rural areas.
Fathers with formal education know better about proper child feeding and hygiene practices, which contribute positively to preventing child stunting.
The study also found maternal BMI has significant influence over the likelihood of stunting, compared to a child born from a normal or obese mother, a child from a thin mother is more likely to have a worse stunting in both urban and rural areas. As Maternal BMI is influenced by maternal nutrition, in order to improve child growth, proper nutrition is essential for the mothers during the prenatal and postnatal period. Healthier mothers have less risk of having stunting children [23]. This is also supported by the study conducted in Ethiopia [8] and Colombia school children [1].
Sex of the household head does not seem to have a sizeable influence over the likelihood of stunting in both residences. The study indicates that household wealth has significant influence on child stunting. Children from the poorest households are more likely to be stunted than those from middle, richer, and richest households both urban and rural areas.
The progressive decline in the prevalence of stunting with an advance in household wealth in both urban and rural areas is an indication of the presence of inequality in stunting in both areas. This study also found that region of residence has a significant influence on child stunting. Amhara, BenishangulGumuz, Affar, and Dire Dawa are most highly affected by child stunting (41-46%). A child living in Tigray has a higher risk of child stunting compared to a child in Addis Ababa, Oromia, Somali, SNNP and Gambella. Region of residence did not show a differential impact on stunting in both urban and rural areas, that is, a significant difference was not observed between the regions within the two residences.
There was a significant difference in the proportion of stunted children across the five socioeconomic categories. The inequality was pro-poor socioeconomic inequality, such that the lower socioeconomic groups were more likely to be stunted and carry a higher burden of the problem than the higher socioeconomic groups. The findings were consistent with the reports of previous studies done in similar settings, Studies that were done in Ethiopia [17], in India [26], and Iran [15] also reported a pro-poor socioeconomic inequality in stunting among under-5 children. Generally, stunting is pro-poor condition particularly in developing countries [20]. They suggested that socioeconomic inequality has significant negative impact on child stunting. The wealth related inequality in stunting is the worst among births to mothers having a secondary and above level of education.
The study found that socioeconomic inequality in stunting in terms of the area of residence urban children in the lowest socioeconomic groups were suffering from greater burden of stunting compared to the rural ones, that is the gap in the level of stunting between affluent households and the poor is much wider in urban areas than rural households. The results of this study have revealed that socioeconomic inequality in stunting varied across the regions of Ethiopia.
The inequality is absent in three regions, that is, Afar, Somali, and Gambela. Addis Ababa is hard hit by the wealth related absolute inequality in stunting.
The results of the decomposition analysis shows that urban rural gap in the prevalence of stunting (13.7%) is decomposed into endowment and coefficient effects. The multivariate decomposition analysis revealed that a significant proportion of the gap in stunting (11.3%) is explained by compositional effects (82.8%). Differential effects of characteristics in urban and rural areas accounted 17.2%, that is, a 2.4 percentage point difference.
That is differences in observed characteristics (or endowments) explain about 82.8% of the difference in children’s stunting gaps between rural and urban areas and difference in the effect of the coefficients (coefficients effect) explain about 17.2% of the gaps, of which 36.7% maternal characteristics, 31.7% household characteristics and 13.6% child characteristics which is done by normalization of characteristics into three groups (Maternal, household and child characteristics).
This is consistent with the reports of previous studies in Bangladesh and Nepal [30], in Ethiopia [31] and in Egypt, Jordan and Yemen [24].
The detailed decomposition result shows that the ruralurban gap is mostly explained by wealth differences 31.9%. Moreover, differences in maternal education 26.7% and Partner’s education 7.1%, Child age 7.9%, Birth order and BMI of the mother 6.3% also have strong influences on this divide. Other determinants including mother’s age, Religion of the mother, birth order, Sex of the household head, and Age at first birth had minimal or no contribution to the inequality in stunting prevalence. The quantification of the contribution of individual socio-economic determinants to rural urban disparities can be used to assess the returns to different types of interventions.
Rural-urban gaps largely accounted for by differing levels of covariates, suggesting that bridging rural-urban inequality in stunting a matter of equalizing endowments of the determinants of nutrition. Our results also suggest that much of this can be achieved by focusing on wealth index, maternal education, child age and spouse’s education.
The multilevel linear regression model result shows that age of child in month, maternal education, maternal age and place of residence were significantly associated to wealth related propoor inequality in stunting in Ethiopia.
Finding from this study are consistent with previous studies conducted in Nigeria [2], Indonesia [10] and Bangladesh [13]. The findings of this study further show that Among the first level variables age of child and the mother and maternal education were found to have a contribution to the wealth related propoor inequality in stunting. From among the context variables it is only place of residence that predicted the inequality in stunting. Pro poor child inequality in stunting was found to be wider in among urban children than rural children. The risk of inequality in stunting is higher among older infants (6-11 months) and children of age above 1 year as opposed to young infants (<6 month). Wealth related inequality in child stunting was more explained by child born to older women than younger mothers. Children born to educated women secondary and above were severely affected by the inequality in stunting than children of uneducated women.
Conclusion
The methodology employed in this paper allows us to determine level of inequality in stunting and its determinants and also decompose rural-urban differences in child stunting into covariate and coefficient effects and further enables us to quantify the contribution of individual explanatory variables (socioeconomic characteristics) to rural-urban differences.
The findings from this study confirm the existence of socioeconomic inequality in stunting in Ethiopia. Findings of this study suggest that child stunting was mainly concentrate among the poor socioeconomic groups. The study found a significant pro- poor socioeconomic inequality in stunting among under five children in Ethiopia, with an 18% stunting gap between the richest and the poorest socioeconomic groups. Maternal education status, age of child in months and mother’s age at first birth were significantly associated factors to the inequality in stunting between the richest and the poorest socioeconomic groups.
The decomposition of rural-urban differences into covariate and coefficient effects shows that the covariate effect is dominant. A core set of determinants wealth index (which incorporates ownership of assets and access to sanitation and drinking water), maternal education and spouse’s education accounts for a very large proportion of the covariate effects. This suggests that there are no fundamental differences in the socioeconomic determinants of child stunting in rural and urban areas. Rural urban disparities in child stunting are primarily attributable to the difference in levels of critical determinants. Our analysis suggests that public health interventions aimed at overcoming rural-urban disparities in child stunting need to focus principally on bridging gaps in socioeconomic endowments and improving the quality of rural infrastructure. Stunting disproportionately affected the rural and the poorest socioeconomic groups in Ethiopia.
Accordingly, intervention measures that entail redistribution of wealth, and improving access to healthcare, clean water and sanitation in rural areas would be effective to reduce the urban rural inequalities in child stunting. Further research is needed in this area. This paper provides the foundation for policymakers to facilitate and support multi sectoral approaches in tackling stunting and achieving equity oriented universal health coverage.
Recommendations
In order to formulate policies to control the child stunting in Ethiopia, it is important not only to understand the incidence of stunting among the children, but also how it differs with geographical categories, demographic and socioeconomic characteristics. In response to this challenge, this study suggests the following possible solutions to reduce child stunting more in Ethiopia.
• Policies that promote parental education, maternal and child care, facilities like source of drinking water and sanitation should be promoted. • Any intervention by governmental and non-governmental organizations that aim at improving under-five children nutritional status should consider the economic classification of the society and geographical categories independently so as to avert under-coverage of the areas that deserve it. • Further studies, should be conducted to identify other determinants and level of inequality in stunting among under-five children to make the declining fast enough.
References
- Abrams B, S Selvin. Maternal Weight Gain Pattern and Birth Weight. Obstetrics and gynecology. 1995; 86: 163–169.
- Akombi, Blessing J, et al. Trends in Socioeconomic Inequalities in Child Undernutrition: Evidence from Nigeria Demographic and Health Survey (2003 – 2013). 2019; 1-13.
- Amare, Zerihun Yohannes, Mossa Endris Ahmed, Adey Belete Mehari. Determinants of Nutritional Status among Children under Age 5 in Ethiopia : Further Analysis of the 2016 Ethiopia Demographic and Health Survey. 2019; 1-11.
- Anwar, Tarique, Paramita Debnath, Balhasan Ali. Decomposing Socio-Economic Inequalities in Nutritional Status among Siblings in High and Low Fertility States of India: International Journal of Health Sciences and Research. 2019; 9: 183–193.
- Dasgupta, Aparajita et al. Assessment of under Nutrition with Composite Index of Anthropometric Failure (CIAF) among under-Five Children in a Rural Area of West Bengal. Indian Journal of Community Health. 2014; 26: 132–38.
- EDHS. 2016. Ethiopia Demographic and Health Survey 2016.
- EMDHS. 2019. Ethiopia Mini Demographic and Health Survey
- Fantay Gebru K, et al. Determinants of Stunting among UnderFive Children in Ethiopia: A Multilevel Mixed-Effects Analysis of 2016 Ethiopian Demographic and Health Survey Data. BMC Pediatrics. 2019; 19:1-13.
- FDRE. 2016. Federal Democratic Republic of Ethiopia. National Nutrition. (July 2016).
- Fikru, Muhammad, Eddy Van Doorslaer. SSM - Population Health Explaining the Fall of Socioeconomic Inequality in Childhood Stunting in Indonesia. SSM - Population Health. 2019; 9:100469. https://doi.org/10.1016/j.ssmph.2019.100469.
- Garrett, James L, Marie T. Ruel. Are Determinants of Rural and Urban Food Security and Nutritional Status Different? Some Insights from Mozambique.” World Development. 1999; 27: 1955-1975.
- Hirvonen, Kalle. Rural-Urban Differences in Children’s Dietary Diversity in Ethiopia A Poisson Decomposition Analysis. 2016.
- Huda,Tanvir M, Alison Hayes, Michael J Dibley. Social Determinants of Inequalities in Child Undernutrition in Bangladesh : A Decomposition Analysis. 2020; (August 2016): 1-12.
- J ayawardena, Priyanka. Socio-economic determinants and inequalities in child socio-economic determinants and inequalities. 2017.
- Kia, Abdollah Almasian, Sahar Goodarzi, Heshmatollah Asadi. A Decomposition Analysis of Inequality in Malnutrition among under Five Children in Iran : Findings from Multiple Indicator Demographic and Health Survey, 2010. 2019; 48:748-757.
- Magadi, Monica A. Household and Community HIV/AIDS Status and Child Malnutrition in Sub-Saharan Africa: Evidence from the Demographic and Health Surveys. Social Science and Medicine. 2011; 73:436-46.
- Mohammed, Shimels Hussien, Fatima Muhammad, Reza Pakzad, Shahab Alizadeh, et al. Socioeconomic Inequality in Stunting among under 5 Children in Ethiopia : A Decomposition Analysis. BMC Research Notes: 2019; 1–5. https://doi.org/10.1186/ s13104-019- 4229-9.
- Mostafa Kamal SM. Socio-Economic Determinants of Severe and Moderate Stunting among under-Five Children of Rural Bangladesh.” Malaysian Journal of Nutrition. 2011; 17:105-118.
- Ntenda, Peter Austin Morton, Ying Chih Chuang. Analysis of Individual-Level and Community-Level Effects on Childhood Undernutrition in Malawi. Pediatrics and Neonatology. 2018; 59:380- 389. https://doi.org/10.1016/j.pedneo.2017.11.019.
- Poel, Ellen Van De, et al. International Journal for Equity in Malnutrition and the Disproportional Burden on the Poor : The Case of Ghana. 2007; 12:1-12.
- Socioeconomic Inequality in Malnutrition in Developing Countries. 044800(April). 2008.
- Rakotomanana, Hasina, Gates GE, Deana Hildebrand, Stoecker BJ, et al. Determinants of Stunting in Children under 5 Years in Madagascar. Maternal and Child Nutrition. 2017; 13.
- Sarma, Haribondhu, Jahidur Rahman Khan, Sayeeda Tarannum. Factors Influencing the Prevalence of Stunting Among Children Factors Influencing the Prevalence of Stunting Among Children Aged Below Five Years in Bangladesh. (July 2017). 2019.
- Sharaf, Mesbah Fathy, Ahmed Shoukry Rashad. Regional Inequalities in Child Malnutrition in Egypt, Jordan, and Yemen: A Blinder-Oaxaca Decomposition Analysis. Health Economics Review. 2015; 6. http://dx.doi.org/10.1186/s13561-016-0097-3.
- Regional Inequalities in Child Malnutrition in Egypt, Jordan, and Yemen: A Blinder-Oaxaca Decomposition Analysis. Health Economics Review. 2016; 0–11. http://dx.doi.org/10.1186/s13561- 016-0097-3.
- Singh, Shrikant, Swati Srivastava, Ashish Kumar Upadhyay. SocioEconomic Inequality in Malnutrition among Children in India : An Analysis of 640 Districts from National Family Health Survey. 2019; 0: 1-9.
- Sinning, Mathias, Markus Hahn, Bauer TK. The Blinder-Oaxaca Decomposition for Nonlinear Regression Models. Stata Journal. 2008; 8:480-492.
- Smith, Lisa C, Ruel MT, Aida Ndiaye. Why Is Child Malnutrition Lower In Urban Than Rural Areas ? Evidence From 36 Developing Countries. 2004; 176.
- Srinivasan, Chittur S, Giacomo Zanello, Bhavani Shankar. RuralUrban Disparities in Child Nutrition in Bangladesh and Nepal. 2013; 1-15.
- Srinivasan, Chittur, Bhavani Shankar. Rural-Urban Disparities in Child Nutrition in Bangladesh and Nepal. 2014. (June 2013).
- Tadesse, Sebsibe, Yinges Alemu. Urban-Rural Differentials in Child Undernutrition In. 2015; 7:15-23.
- Tadesse, Sebsibe Yinges Alemu2. Urban-Rural Differentials in Child Undernutrition in Ethiopia. 2015.
- Takele, Kasahun, Temesgen Zewotir, Denis Ndanguza. Understanding Correlates of Child Stunting in Ethiopia Using Generalized Linear Mixed Models. 2019; 1-8.
- Twisk, Jos WR. Explaining Differences between Groups. Applied Mixed Model Analysis (Oaxaca): 2019; 78–89.
- Unicef/ WHO/The World Bank. Levels and Trends in Child Malnutrition. 2018; 1-16.
- Levels and Trends in Child Malnutrition - Unicef WHO The World Bank Joint Child Malnutrition Estimates, Key Findings Pf the 2019 Edition. Unicef: 2019; 4. http://www.unicef.org/media/ files/JME_2015_edition_Sept_2015.pdf.
- Van de Poel, Ellen, Owen O’Donnell, Eddy Van Doorslaer. Are Urban Children Really Healthier? Evidence from 47 Developing Countries. Social Science and Medicine. 2007; 65: 1986-2003.
- Van Doorslaer, Eddy, Owen O’Donnell. Health Inequality and Development Measurement and Explanation of Inequality in Health and Health Care in Low-Income Settings. 2011.
- Wemakor, Anthony, et al. Young Maternal Age Is a Risk Factor for Child Undernutrition in Tamale Metropolis, Ghana. BMC Research Notes: 2018; 1–5. https://doi.org/10.1186/s13104- 018- 3980-7.
- WHO. World Health Organization in Ethiopia Anual Report. 2017.