
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Assessment of knowledge, atitude and practice towards legalization of abortion among child bearing age women, in Chichu Dilla Zuria Woreda, SNNPR Gedeo zone, South Ethiopia, 2020
Yetayale
College of Health Sciences, Dilla University, Dilla, SNNPR, Ethiopia.
*Corresponding Author: Yetayale
College of Health Sciences, Dilla University, Dilla,
SNNPR, Ethiopia.
Email: yetalb@yahoo.com
Received : Feb 25, 2022
Accepted : Apr 11, 2022
Published : Apr 18, 2022
Archived : www.jcimcr.org
Copyright : © Yetayale (2022).
Abstract
Background: Septic abortion is the most common cause of maternal morbidity and mortality, especially in developing countries, even if safe methods are available. This research is expected to solve the problems of women’s knowledge, attitudes and practice, and add some knowledge to make better use of services.
Objective: To evaluate knowledge attitude and practice to wards legalization of abortion among child bearing age women in chichu dilla zuria woreda, Gedeo zone South Ethiopia.
Methodology: A community-based cross-sectional study was conducted at Chichu Dilla Zuria Woreda SNNPR from June to July 2020. Use pre-tested structured questioners, and. A total of 422 women of childbearing age were randomly sampled from Chichu woreda, Dilla Zuria South Ethiopia.
Results and discussion: A total of 420 interviewees were included in the study, most of them were married, housewives, and illiterate. Gedio is the first for the ethnic minority Group as compared to South Ethiopia zones or the so-called state, and the Orthodox Church is one of the main religions or as compared to other religion majority of the people follower of orthodox Christian. This study shows that there is a knowledge gap in abortion, and a considerable number of women have a negative attitude towards legalized abortion.And a large number of individuals-10.1percent still practice unsafe abortions.
Conclusion and recommendations: Based on the results of the study, it can be concluded that there is a wide knowledge gap among chichu woreda women’s of childbearing age and a negative attitude towards the legalization of abortion. Finally, I recommend all stakeholders to the Woreda Health Office; includes the health center staff to make better efforts and strong health education to reduce the morbidity and mortality of pregnant and lying-in women.
Keywords: Knowledge; Attitude; Practice; Legalization abortion; Women’s child bearing; South Ethiopia.
Citation: Yetayale. Assessment of knowledge, atitude and practice towards legalization of abortion among child bearing age women, in Chichu Dilla Zuria Woreda, SNNPR Gedeo zone, South Ethiopia, 2020. J Clin Images Med Case Rep. 2022; 3(4): 1797.
Introduction
Abortion is the termination of a pregnancy before it reaches viability (less than 28 completed weeks in Ethiopia). It can be classified as safe or unsafe septic, therapeutic, etc. On the other hand, it can also be divided into induced and spontaneous [3]. Abortion is one of the most common causes of maternal morbidity and mortality and is therefore the most important public health problem worldwide. Due to the multitude of social and economic problems, as well as due to inadequate provision of services, women find their own way to alleviate their problems, which increases the risk and may even lose their lives [1]. The problem is clear and diverse in developing countries. There are about 4 million unsafe abortions in Africa, of which 1/3 of deaths occur every year.
Among the various direct and indirect causes of maternal mortality, septic abortion is the most common one in the world [1] Ethiopia, one of the developing countries where FP services with low coverage (22.9) and induced abortion are illegal if not done for protection child. The mother’s life and certain criteria do not currently correspond to the days of induced abortion. The problem is especially in urban areas, where the socio-economic pressure on space and birth control in general is high [9].
Statement of the problem
Maternal health is one of the major indicators and parameters of development worldwide, with one in six women of childbearing age lacking information and access to the full range of modern contraceptive methods. And about 38% of all pregnancies are not desired each year. In the midst of this unwanted termination of pregnancy, millions of abortions occur each year, between 40 and 60 million each year [11]. According to WHO 50 million pregnancies end each year, of which about 20 million are unsafe. This is done by people who lack skills, at least where they do not meet the minimum medical standards, or both. 70,000 women die each year as a result of unsafe abortions, hundreds of thousands more are seriously injured, often with permanent disabilities each year, and more than 200 women die from unsafe abortions [2]. The problem is clearly visible in Africa, where approximately 4 million unsafe abortions are performed each year and where 1/3 of all deaths are from unsafe abortions. With Ethiopia being one of the developing countries, it is pretty clear that unsafe abortions are due to a lack of information and access to contraception. In some situations, abortion is accepted by some people because political and medical attitudes towards induced abortion have helped improve the philosophy of change [16]. Research shows that in Ethiopia only 14% of the reproductive age group use contraceptives. 42% of all pregnancies in 2008 were unwanted. Ethiopia has performed 382,500 abortions, and 23 abortions per 1,000 women each year, only 27% are legal and safe in medical institutions. In the same year, 58,600 women received treatment for abortion-related complications caused by unsafe abortions. Among them, 100 women died of complications, more women suffered related injuries or diseases, and 4 out of 10 showed signs of infection and invasive injury when they arrived at the medical facility. Many women with complications never arrived at the medical facility or Healthcare institutions. Some religious concepts remain unchanged, leading to personal, medical, and political conflicts [3]. In most countries in the world, termination of pregnancy is only allowed under certain circumstances, but this policy does not properly deal with abortion issues. Therefore, this study will aim to evaluate women’s knowledge, attitudes and practices regarding the legalization of abortion and the application of safe abortion care. The results of this study will help promote abortion practices, increase women’s acceptance of abortion, and reassess the low level of abortion in our country.
Methodology
Study area, period and design
An institution-based cross-sectional study was conducted from February to July 2020 in Chichudilla zuzria Woreda, Gedeo Zone, and SNNPR. EC Chichu is located 365 km southwest of the capital Ethiopia (Addis Ababa) and 95 km of the provincial city SNNPR (Hawassa). And it is far 5 km from the town of Dilla. The total population of the town was estimated to be 10,106. The town is divided into 6 sub-kebles. Dilla Zuria Woreda Dilla Town and Sidama Zone in the north, Gangoa Woreda in the Oromia region in the west, Gedeo Zone Woreda Worba in the south, and Gedeo Zone Bureholla in the east. Most of the religions that cross the district from to Moyale consider the district to be a Protestant orthodox and Muslim. The Ethiopian people’s economy is based on agriculture, the work and trade of everyday workers. The main cash crops in society are coffee, various fruits, corn, fake bananas (kocho) and bananas.
Sampling procedure
A multi-stage sampling procedure was used to include a representative sample of 489 randomly selected women of childbearing age for this study. In the first stage, three of the nine Kebeles were selected at random using the lottery procedure. After the initial starting households have been determined on the basis of random numbers, individual households in the selected Kebeles are selected using a systematic sampling procedure. The sample size is assigned to each Kebele in relation to the family size of the Kebel. The households in each selected Kebele are determined by the Kebele Bureau, and the number of households contained in the selected Kebele is determined in proportion to the household size. Adults from selected families are further selected and interviewed. If there is more than one eligible participant in the household, only one will be selected by lottery procedure. The sample size is determined using a single population ratio formula.
Data collection procedure
The English version of the interviewer management structured questionnaire was adapted from the literature by the investigators. It was then translated into Amharic, which is the official working language of the study area (Ethiopia). The English teacher at Dilla University checked the consistency of the translation from English to Amharic. Before starting data collection, 5 people were recruited from the Dilla referral hospital for data collection. Among them, there are 2 psychiatric nurses, 2 administrative staff, and 1 supervisor. In order to maintain the quality of the data, data collectors and supervisors received a one-day training that involved the necessary explanation of the research and how to answer any questions raised by the interviewees. Pre-testing of 25 adults not included in the study
Study variables and measurements
The study assessed participants’ knowledge and attitudes towards the legalization of safe abortion. The knowledge of women of childbearing age about safe abortion scores is calculated from 8 knowledge-specific questions with a high degree of internal consistency (Cronbach’s alpha = 0.712). According to the respondent’s answers, each correct answer gets one point, and the wrong answer gets zero points. Lastly, respondents with a score of 60% or higher on knowledge questions are considered to have “good knowledge”, and respondents with a score of less than 60% are considered to have “bad knowledge” was considered. Women of childbearing age attitudes towards a safe abortion score were calculated from 11 specific questions with high internal consistency (Cronbach’s alpha = 0.706). Likert five-point scale, coded as 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree, and then divided into “agree” (strongly agree and agree) and “disagree” “(Strongly disagree, disagree and neutral). Respondents with scores greater than or equal to the average score are considered to have “favorable attitudes”, and respondents with scores lower than the average score are considered to have “unfavorable attitudes” []. The independent variables are age, gender, religion, marital status, previous place of residence (urban or rural), year of study, and household income.
Data quality control
Pre-testing of the data collection tool was conducted on 5% (39 participants) of the study participants who were female of childbearing in Dilla Town. Data collectors were trained prior to data collection, data collection procedures, ethical considerations, data quality control, and confidentiality. Prior to the start, respondents were informed about the purpose of the survey and the importance of voluntarily participating in the survey. The data collected was checked daily for integrity and consistency. Data is stored in a personal protected location and confidentiality is guaranteed by not recording personal identifiers
Statistical analysis
The data has been sanitized, encoded and entered into the Epi data version 3.1. This data was then exported to SPSS version 20 for analysis. For some variables, descriptive statistics such as frequency, percentage, mean, standard deviation were calculated. The data presentation was done using frequency distribution tables. A Generalized Linear Model (GLM) called logistic regression was used to identify factors influencing student khat chewing behavior. Binary logistic regression coefficients were estimated by Wald statistics. Odds ratio [expo (β)] of the logistic regression coefficients indicates the probability of an increase (OR> 1) or decrease (OR <1) in khat chewing when treated with various explanatory variables. The cutoff point for the bivariate logistic regression was set at p <0.25 in order to include variables in the multivariate logistic regression. Statistical significance is confirmed if the p-value is less than 0.05.
Ethical approval
This study was conducted with the official permission of the Department of Psychiatry and is an ethical accreditation obtained from the Research and Institutional Review Board of the University of Dila with the Manager of the Faculty of Health Sciences and the Dean of the Faculty of Health Sciences and Medicine of the University of Dila. I got in touch. Date collection was done after oral consent from each respondent. Similarly, respondents’ confidentiality was maintained and the information provided by respondents was used only for research purposes.
Result and discussion
Sociodemographic analysis
Data were collected from 420 respondents from Chichu. The average age of the subjects was 28.79 years. In terms of educational status, 20.3% participated in the first cycle, 33.5% in the second cycle, 27.7% in high school and 18.5% are illiterate. With regard to marital status, more than half, or 68%, were married. Most of the study participants, 62.3% were Orthodox Christians by faith and 82.49% Gedieo by ethnicity. About 49.2% of the subjects of the study were housewives, 27.8% were farmers, 13.4% were private workers, 3.2% were civil servants, and 6.4% were day laborers. Among the study participants, 33.7% did not have a regular monthly income, and 32.8% had less than 500.00 et-birr per month (Figures 1,2 and Table 1).
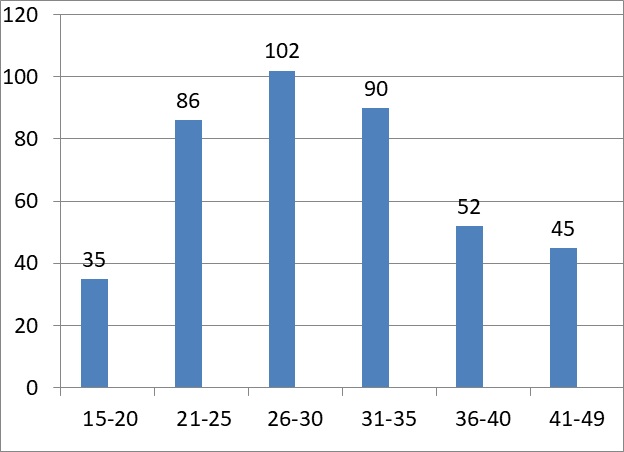
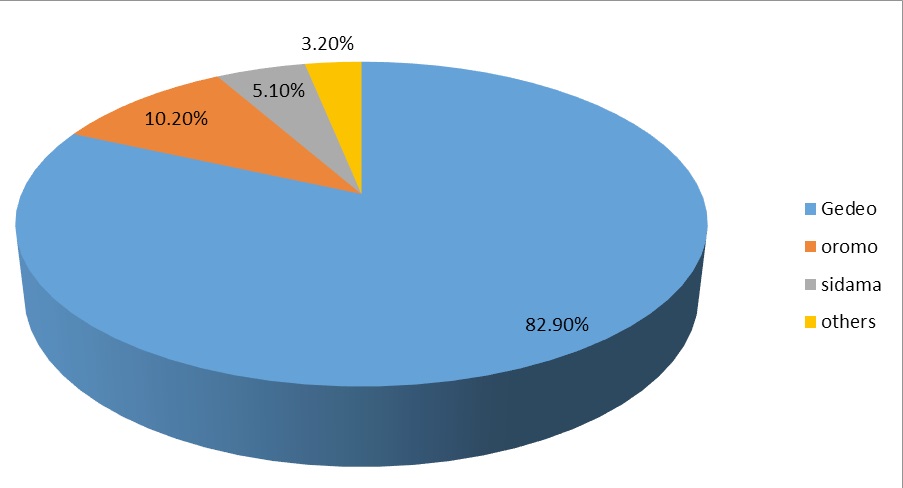
Table 1: Shows socio demographic characteristics of the respondents of chichuDillazuria, South, Ethiopia; June 2020.
Socio demographic characteristics |
Frequency |
Percent % |
|
Educational status |
Cycle one |
84 |
20.3 |
|
Cycle two |
138.5 |
33.5 |
|
High school |
113 |
27.5 |
|
Illiterate |
78 |
18.5 |
Marital status |
Married |
286.6 |
68 |
|
Single |
83.58 |
19.9 |
|
Divorced |
34.86 |
8.3 |
|
Widowed |
32.76 |
7.8 |
Occupation |
Ho use wife |
206.64 |
49.2 |
|
Farmer |
116.76 |
27.8 |
|
Private workers |
56.2 |
13.4 |
|
Government employer |
13.44 |
3.2 |
|
Daily laborer |
26.9 |
6.4 |
Income status |
<500 |
138 |
32.8 |
|
501-1000 |
43 |
10.2 |
|
1000-1500 |
59 |
10.4 |
|
>2000 |
24 |
5.8 |
|
No regular income |
141.5 |
33.7 |
Religion |
Orthodox |
226.4 |
53.9 |
|
Protestant |
135 |
32.2 |
|
Muslium |
36 |
8.5 |
|
Others |
39 |
9.2 |
Knowledge attitude and practice analysis
Most of the respondents, 78.3, did not read health brochures or other written material. The majority of respondents get health information from the radio. However, 84.4% of the respondents did not know that there are few abortions in our country. From those who know the country's abortion lows, the majority of respondents, 65.5%, said the lows did not address the issue of women. 73.3% disagree with the need to correct the low majority of respondents. 23.2% of respondents need to revise their lows (Table 2).
Table 2: Shows source of information of the respondents of cichuDillazuria, South, Ethiopia; June 2020.
Source of information |
Frequency |
Percent % |
Radio |
216.8 |
51.6 |
Health professionals |
115 |
27.4 |
Television |
68 |
16.6 |
Others |
18 |
4.3 |
Most of the respondents, 78.3, did not read health brochures or other written material. The majority of respondents get health information from the radio. However, 84.4% of the respondents did not know that there are few abortions in our country. From those who know the country's abortion lows, the majority of respondents, 65.5%, said the lows did not address the issue of women. 73.3% disagree with the need to correct the low majority of respondents. 23.2% of respondents need to revise their lows (Table 2).
Regarding the reason for their opinion, those interviewees who think abortion should continue, because abortion contradicts the fall of God, it is sin, and it may eventually lead to many complications, such as infertility. The reason it should be legal whenever needed is that even if it is illegal, if a woman faces an unintended pregnancy, she may take her own unsafe measures, and unsafe measures may kill the woman and cause complications. The reason for flexibility is that the legalization of freedom may cause women to make inadequately thoughtful decisions, and restrictions may also cause women to take unsafe measures. Therefore, it should be flexibly changed according to the situation.
90.8% of respondents believe that legalized abortion can reduce septic miscarriage, 4.2% of respondents do not believe it, and 5% of respondents do not know the difference.
The current practice of low abortion in my country is supported by the majority of respondents, 74.7% and 25.3% do not support it. The reason for the lack of support is that the low level does not adequately solve the female problem.
Regarding unintended pregnancies, a considerable number of women face unintended pregnancies, 26.8% and 73.2% respectively. As a result, 10.1% of women terminated unintended pregnancies in traditional ways, 1.3% terminated in medical institutions, and 15.4% did not even want to have it.
Discussion
Knowledge assessment and attitudes towards legalization of abortion in the childbearing age group are important to minimize the burden associated with unsafe abortion. This study revealed that the overall knowledge of safe abortion was 84.4%. This finding is consistent with other studies conducted in Kampala, Uganda [17], and it is recorded that 72.4% of the childbearing age group had sufficient knowledge of safe abortion. Nonetheless, our findings were at Mek'ele University in northern Ethiopia [18] and Sodo University in southwestern Ethiopia [19], where student knowledge scores were reported at 44.4%, 38.9%, and 36.4%, respectively. It was higher than the results of the studies conducted. When it comes to women's attitudes, quite a few women have shown a negative attitude towards the legalization of abortion, even if it has a negative impact on their lives. The reason for this contradiction may be due to differences in research participants. On the other hand, in our survey, survey participants included only the age of childbirth. It is true that their awareness will increase and the knowledge level of female community members will also increase [20]. In addition, variations can occur due to differences in access to health information in different settings. This study showed that 90.42% of female students at the University of Mizan Tepi in southwestern Ethiopia have sufficient knowledge about safe abortion [21], a greater discovery than this one. In the current study, it was found that women in the 25-year-old and above age group were 2.89 more likely to have sufficient knowledge about safe abortion than women in the 18-19-year-old age group. This finding is similar to a cross-sectional study conducted in Kampala, [22]. A possible clarification may be the fact that with age, exposure to information about safe abortion may also increase. The study also shows that women who give birth from urban areas are more knowledgeable than women who live in rural areas. This may be due to urban residents having access to information and educational media. Respondents whose parents are literate are more than three times more likely to have a good understanding of safe abortion. This finding has received more support from the study of Mekelle University, [18]. This may be because the parents have a high educational background, which allows their children to know the additional and important lessons in addition to the academic program. This study showed that women carrying children who had heard of safe abortion were more likely to have good knowledge and practices than those who had not heard of safe abortion. This result is consistent with other studies conducted in Mizan Tepe University, Southern Ethiopia [21] and South Africa [23]. The reason may be that women of childbearing age, who have varied information about the health problems associated with unsafe abortion, may have raised awareness of serious barriers to their education and other health problems. In addition, women who are carrying a child are becoming more available in various media and receive more information about the problem, which may have given good knowledge about safe abortion. In addition, women in labor who have greater access to safe abortion health education could raise awareness about abortion, which could further enhance their knowledge of safe abortion.
Conclusion
From analysis of results obtained it can be concluded as follow:
• Safe abortion practices are not completely successful as a national program. This study found that women in the childbearing age group of the Chichu community showed low levels of knowledge, negative attitudes and practiced unsafe abortion towards legalization of abortion. Sh. And also this study revealed that one-thirds of participants had good knowledge and few of the participants had a favorable attitude regarding safe abortion, but, still, a significant proportion of women in the childbearing age group had poor knowledge and unfavorable attitude towards safe abortion. In addition, student age, location, family education, and abortions ever heard were factors associated with knowing about safe abortions. The age of the students and residents was related to attitudes towards abortion. Therefore, information, education and communication programs on reproductive health of young people should be provided to address topics related to safe abortion for all college students. There is a need to have forums and panel discussions on safe abortion, especially among youth and students from rural areas. A large number of women still perform unsafe abortions in traditional ways. This can lead to complications and may lead to maternal illness and even death.
Recommendations
The study that conducted on the assessment of knowledge attitude and practice to wards legalization of abortion shows that problems like knowledge gap poor utilization of safe abortion service. So that we recommended the following points in order to improve and increases awareness and utilization.
I recommend Dilla zuria woreda health office working to create awareness about safe abortion practice.
I recommend chichu health center Promoting and educating the community about the importance of safe abortion practice which has effect on maternal morbidity and mortality
Declarations
Consent for publication: Not applicable.
Availability of data and materials: The data that support the findings of this study has a sort of identifier of individual participants and researcher reserved to send it. Competing of interest: All of the authors declare they have no conflict of interest.
Funding: Not applicable.
Author contributions: YB has contributed in idea conception, topic selection, and writes up of proposal for funding. AE has contributed idea generation in title selection, contributed in organizing literatures important to the study, commented both proposal draft and result and involved in data collection and analysis of data and in writing the manuscript. Finally all authors read and approved the final manuscript for publication.
Acknowledgments: The author would like to thank Dilla University, respondent author, Data collectors for their responsible data collection and few individual who were helping the primary author in manuscript preparation.
References
- Ahimed A. A retrospective study of the admission of abortions at Jimma Hospital in southern West Ethiopia. Medical journal. 1996; 10
- Martha Jarnell, Tase Dowid, Ortiz Mariscal, Judy Fuinklem, Study Guide.
- Kebedes (ID, Jira C. (bachelor, master of health), W / mariam D (MD, research on illegal abortion at Jimma Hospital in southwestern Ethiopia, medical journal April 1994; 32).
- Low Safe Abortion Practices and WHO Health Policy Guidelines, Geneva, 2003.
- Wikipedia, low abortion rate, encyclopedia.
- Unpublished research paper by Asamenev Belay on the quality of delivery services in the city of Gonder.
- Sir David E. Impact of legal abortion on public health. 2003; 35.
- Bitler M, the Plant M. Sexual and Reproductive Health Perspective. 2002; 34.
- Clix J. An Economic Analysis of the Abortion Policy Review.
- Handbook O. Reproductive Health of the Ethiopian Health Center Team. Cooperation with Carter Center. 2003.
- Benoa RKO, Hussey M. MP World Abortion Estimate. 1994; 1-7.
- Mekbis “T” (Doctor of Medicine, PhD). Use condom treaty catheterization to prevent miscarriage.
- Georgia W. Life torig. 2000; 1-2.
- Health profile ESHE project area SNNPR. 1998; EC
- Ethiopian criminal low price. 355
- Introduction to Catholic Free Choice How to talk about abortion.
- Paluku JL, Kalisoke S, Julius W, Kiondo P. Information on adolescents participating in the naguru and healthy female youths’ knowledge and attitudes towards abortion. Center, Kampala, Uganda. J Public Health and Epidemiology. 2013; 5: 178-185.
- Desalegn S, Desta A, G/selassie A, Tesfay A, Abaya R. Knowledge, Attitudes, and Factors Related to Safe Abortion for First-Year Students of Tigray Moore University, Ethiopia. International Journal of Drugs Scientific Research (IJPSR). 2015; 6.
- Gelaye AA, Taye KN, Mekonen T. Severity and Risk Factors of Abortion in Ordinary Female Students at Voletta Sodo University, Ethiopia. BMC Women’s Health. 2014; 2: 50
- Tara A, Norman W. University of British Columbia Undergraduate Medical Students Knowledge Assessment Survey, Vancouver, British Columbia, Canada. 2010.
- Mekuriaw S, Dereje RMA, Kumalo A, Feyissa M. Knowledge, Attitudes and Practice of Safe Abortion among Female Students of Mizan-Tepi University in Southwestern Ethiopia. Women’s Health Journal. 2015; 1: 2167-2420.
- Paluku JL, Kalisoke S, Julius W, Kiondo P. Kampala Naguru Youth Information and Health Center, Kampala, Uganda, Young Women’s Knowledge and Attitudes about Induced Abortion. Journal of Public Health and Epidemiology. 2013; 5: 178-185.
- Wheeler SB, Zullig LL, Reeve BB, Buga GA, Morroni C, et al. The Attitudes and Intentions of South African Medical on Abortion Regulations. International Perspectives on Sexual and Reproductive Health. 2012; 2: 154.