
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
Fortuitously detected Paget’s bone disease in a patient with TENIS syndrome on FDG PET/CT
Ayush Mishra
Laboratory of Biomaterials and Tissue Engineering, Faculty of Medicine and Health Technology, Tampere University, Korkeakoulunkatu 3, 33720 Tampere, Finland.
*Corresponding Author: Ayush Mishra
Laboratory of Biomaterials and Tissue Engineering, Faculty of Medicine and Health Technology,
Tampere University, Korkeakoulunkatu 3, 33720
Tampere, Finland.
Email: maanayush0007@gmail.com
Received : Feb 01, 2022
Accepted : Apr 13, 2022
Published : Apr 20, 2022
Archived : www.jcimcr.org
Copyright : © Mishra A (2022).
Abstract
Papillarycarcinoma thyroid is the prevalent histological subtype of well-differentiated thyroid cancer (WDTC). Patients are treated with thyroidectomy followed by radioactive iodine (RAI) therapy. Follow-up is done with a low-dose whole-body scan (WBS), serum thyroglobulin (sTg), and neck ultrasonography depending upon the stage. Elevated serum sTg despite a negative WBS scan is termed the TENIS (Thyroglobulin elevated negative iodine scintigraphy). FDG PET/CT is indicated in such cases. Here we present an unusual presentation of incidentally detected Paget’s disease bone (PDB) in a WDTC presented with TENIS syndrome.
Keywords: Well-differentiated thyroid cancer; TENIS syndrome; Paget’s disease bone.
Citation: Mishra A. Fortuitously detected Paget’s bone disease in a patient with TENIS syndrome on FDG PET/CT. J Clin Images Med Case Rep. 2022; 3(4): 1799.
Case report
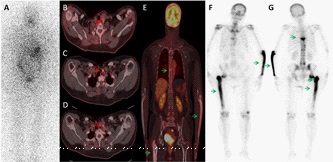
A 74-year-old lady presented with a complaint of progressive neck swelling for two years. FNAC from the swelling was suggestive of papillary carcinoma thyroid (PCT). She underwent total thyroidectomy with central compartment lymph node dissection. Histopathology revealed multifocal PCT with central compartment lymph node metastases. Her baseline stimulated sTg was 5.3 ng/ml after levothyroxine withdrawal. WBS showed uptake in the operative bed (not shown). She was treated with 100 mCi of I-131 and was kept on a suppressive dose of thyroxin hormone. Her sTg gradually increased (77.5 ng/ml) in follow-up after three years. WBS was negative for metastatic disease. She underwent FDG PET/CT, that revealed cervical and upper mediastinal lymph nodes. Apart from that, multiple pagetic lesions were also noted. The patient had a history of mild localized pain and tenderness over these. Her Serum Alkaline phosphatase level was elevated (269 U/L). The patient refused resurgery for cervical lymph nodes. She is on Zolendronic acid infusion and remains asymptomatic. She is in regular follow-up, and her suppressedsTg remains stable even after two years.
Thyroid carcinoma is the commonest malignancy of the endocrine system. The majority belongs to well-differentiated thyroid cancers (papillary and follicular cancer) and are relatively indolent. These have long-term survival in a significant number of nonmetastatic patients. Metastatic thyroid carcinoma is noted in about 10% of patients with papillary carcinoma and up to 25% with follicular carcinoma [1]. The most typical sites for distant metastases are the lungs and bones [2]. The clinical presentation of these patients with differentiated metastatic carcinoma is highly variable. Loss of iodine concentrating capability due to either dedifferentiation or reduction in sodium/iodide symporter expression in postoperative thyroid cancer patients makes iodine inefficientfor imaging and therapy [3]. This entity is called TENIS syndrome. In this group of patients, FDG PET/CT has a decisive role. We present a TENIS patient in whom FDG PET/CT helped to find the disease burden and fortuitously detectedpolyostotic Paget’s disease.
The diagnostic and therapeutic approaches for TENIS syndrome do not have a common consensus. It includes observation, re-surgery, chemotherapy, tyrosine kinase inhibitors, re-differentiation therapy, and others [4]. FDG PET/CT is the well-established imaging modality for disease burden evaluation in TENIS patients [5]. Here, FDG PET/CT incidentally detectedPDB in a WDTC presented with TENIS syndrome. Paget disease of bone (PDB) is the second most common bone remodeling disease, as osteoporosis leads [6]. PDB is a chronic, progressive bone disorder that could involve single (monostotic) or multiple bones (polyostotic). The most commonly involved bones include the pelvis, femur, spine, skull, and tibia [7]. Skeletal lesions of PDB are characterized by increased vascularity, osteoclastic bone resorption and, disorganized increased bone formation [6]. Patients with PDB are often asymptomatic. They are frequently incidentally detected with an elevated serum alkaline phosphatase or on X-rays performed for unrelated reasons [8]. Mazières B et al. highlighted the use of scintigraphy in this disease. It allows the spread of the disease to be diagnosed without doing X-rays of the entire skeleton. In twenty percent of cases, this disease cannot be located using X-rays and is detected by scintigraphy. It also supplies an additional objective criterion for judging the development of this disease, especially under treatment [9]. PDB results in weakened bone strength and abnormal bone architecture, leading to pain, deformity or, depending on the bone involved, fracture in the affected bone. The current mainstay of treatment in PDB is bisphosphonates (disodium pamidronate, alendronate, risedronate). They are potent inhibitors of bone resorption and provide prolonged remission of the disease [10]. This case undoubtful utility of the FDG PET/CT in TENIS syndrome. Being a whole- body hybrid molecular imaging, PET/CT helps to unveil many non- malignant lesions.
FDG PET/CT isa valuable imaging modality in the management of the TENIS syndrome. It could unveil several unrelated incidental pathologies such as PDB along with recurrent thyroid cancaer.
References
- Mazzaferri EL, Kloos RT. Current Approaches to Primary Therapy for Papillary and Follicular Thyroid Cancer. J Clin Endocrinol Metab. 2001; 86(4): 1447-63.
- Mazzaferri EL, Kloos RT. Current Approaches to Primary Therapy for Papillary and Follicular Thyroid Cancer. J Clin Endocrinol Metab. 2001; 86(4): 1447-63.
- Prashar S, Dahiya D, Sood A, Chatterjee D, Kaur R, Mittal BR. Revisiting 99mTc-MIBI Radioguided Surgery in Management of TENIS Syndrome. Clin Nucl Med. 2020; 45(5): e243-4.
- Silberstein EB. The problem of the patient with thyroglobulin elevation but negative iodine scintigraphy: the TENIS syndrome. Semin Nucl Med. 2011; 41(2): 113-20.
- Caetano R, Bastos CRG et al. Accuracy of positron emission tomography and positron emission tomography-CT in the detection of differentiated thyroid cancer recurrence with negative (131) I whole-body scan results: A meta-analysis. Head Neck. 2016; 38(2): 316-27.
- Ralston SH. Pathogenesis of Paget’s disease of bone. Bone. 2008; 43(5): 819-25.
- Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism - Google Books
- Wermers RA, Tiegs RD, Atkinson EJ, et al Morbidity and mortality associated with Paget’s disease of bone: a population-based study. J Bone Miner Res Off J Am Soc Bone Miner Res. 2008; 23(6): 819-25.
- Mazières B, Jung-Rosenfarb M, Bouteiller G, et al scintigraphie osseuse dans la maladie de Paget [Bone scintigraphy in Paget’s disease]. Rev Rhum Mal Osteoartic. 1978; 45(5): 311-6. French.
- Michou L, Brown JP. Emerging strategies and therapies for treatment of Paget’s disease of bone. Drug Des Devel Ther. 2011; 5: 225-39.