
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Paraplegia due to involvement of a long segment of the spinal cord: A rare presentation of chronic myeloid leukemia in blast crises
Avaneesh Shukla1; Shailendra Prasad Verma1*; Somil Jaiswal2; Mili Jain3; Anil Kumar Tripathi1
1 Department of Clinical Hematology, King George’s Medical University, Lucknow, India.
2 Department of Neurosurgery, King George’s Medical University, Lucknow, India.
3 Department of Pathology, King George’s Medical University, Lucknow, India.
*Corresponding Author: Shailendra Prasad Verma
Associate Professor, Department of Clinical Hematology, King George’s Medical University, Lucknow,
UP, India.
Email: spverma1998@gmail.com
Received : Jan 21, 2022
Accepted : Apr 14, 2022
Published : Apr 21, 2022
Archived : www.jcimcr.org
Copyright : © Verma SP (2022).
Abstract
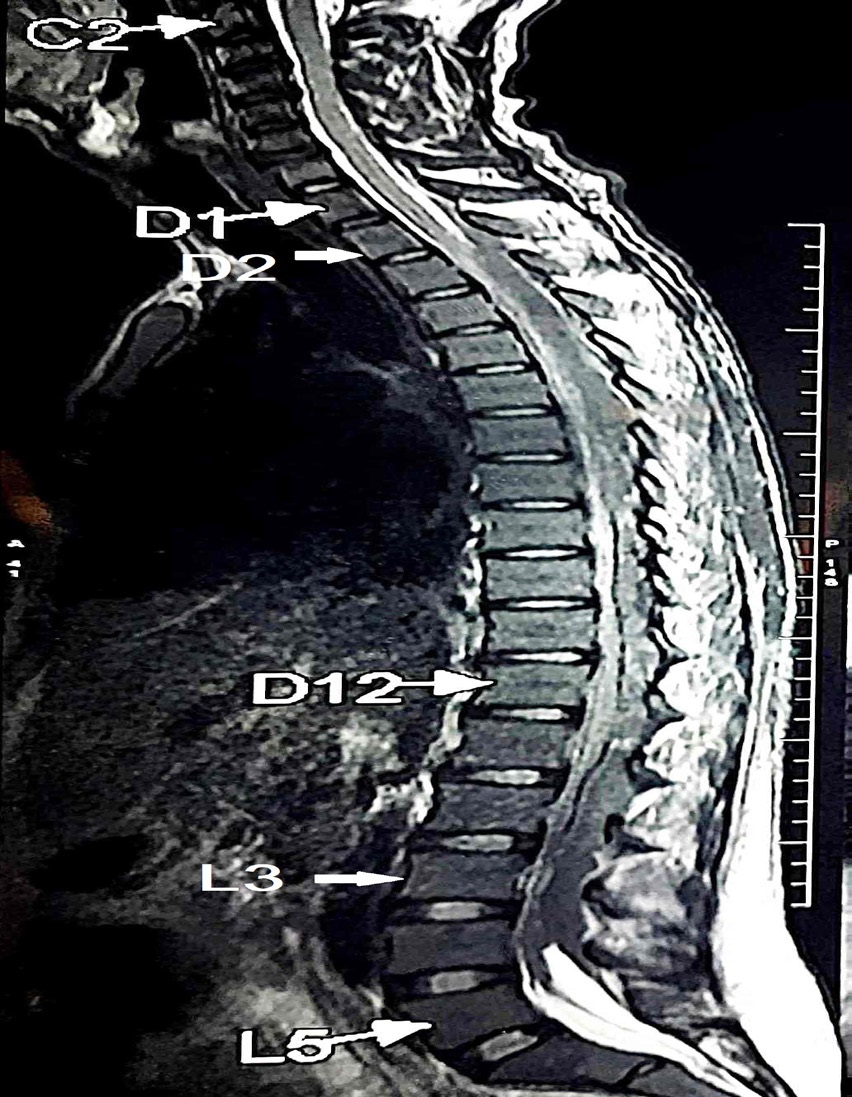
Chronic myeloid leukemia is the most common myeloproliferative neoplasm and very rarely presents upfront with involvement of central nervous system. Here we present a peculiar case of a 34 year old male who presented with complaints of rapidly progressive weakness of both the lower limbs of 2 week duration. On examination it was found to be upper motor neuron type of sensory motor paraplegia with bladder and bowel involvement. The upper level of sensory involvement was at D-6. On further investigations his total leucocyte counts were very high and he was diagnosed as a case of chronic myeloid leukemia in chronic phase. MRI scan of spine was suggestive of extensive involvement of spinal cord from D2-L3 level causing compression over thecal sac & spinal cord leading to the above mentioned complains. Biopsy from the lesion was suggestive of collection of extramedullarly blasts.
Citation: Shukla A, Verma SP, Jaiswal S, Jain M, Tripathi AK. Paraplegia due to involvement of a long segment of the spinal cord: A rare presentation of chronic myeloid leukemia in blast crises. J Clin Images Med Case Rep. 2022; 3(4): 1801.
Introduction
Chronic Myeloid Leukemia (CML) is the most common Myeloproliferative Neoplasm (MPN). Patients usually present with fatigue, abdominal fullness and left upper quadrant pain [1]. The duration of symptoms ranges from several weeks to several months before diagnosis. In the current era of tyrosine kinase inhibitor based targeted therapy, survival is almost similar to general population [2]. Clinically, patients present with prominent splenomegaly. Routine CBC shows marked leucocytosis with shift to left. Acute presentation is very rare in CML especially in Chronic Phase (CML-CP) but patients can present acutely upfront in Accelerated Phase (AP) or Blast Crises Phase (CML-BP). Extramedullary involvement of spinal cord known as granulocytic sarcoma has been reported in acute myeloid leukemia, multiple myeloma, lymphoma and acute lymphoblastic leukemia [3,4]. CML blast phase presenting with granulocytic sarcoma and causing cord compression has been rarely reported [5].
Case report
This patient is a 34 year old male, who presented with complains of mild back ache for 1 month, acute onset progressive weakness of both lower limbs for 2 weeks, unable to walk with loss of bladder and bowel control for one week. Back pain was dull aching in nature and used to aggravate during night. Weakness initially started in right lower limb but soon involver left limb within a span of 2 days. He was bed bound 1 week before admission at our centre. He was referred to department of neurology for evaluation of paraparesis. In view of very high counts he was referred to Clinical Hematology for evaluation and management of suspected leukemia. There was no history of trauma to back, fever, bleeding, pain at other sites, any swellings in body or such episode in past. He had no history of any significant previous illness, co-morbidities or addiction.
At the time of admission vitals were normal. On general examination patient was thin built. Pallor, icterus, edema and lymphadenopathy were absent. Abdominal examination revealed splenomegaly 5 centimetres below left costal margin. Cardiac and respiratoty system examination was within normal limits.
On examination of nervous system he was conscious and oriented to time, place and person. He had power of 0/5 in both lower limbs, bilateral planters were non elicitable, tone was bilaterally reduced, both foot were in dorsiflexed position and deep tendon reflexes including Knee and ankle jerk were absent. Sensory examination revealed loss of pain and temperature upto D-6 thoracic level. Joint pain and position sense were also lost bilaterally. Neurological examination of upper limb and cranial nerves was within normal limits. Urgent neurosurgical consultation was sought. His peripheral smear revealed features of myeloproliferative neoplasm most likely chronic myeloid leukemia. Peripheral blood blasts were 2% and bone marrow aspiation was also consistent with chronic phase. His BCR-ABL test done at admission turned out to be positive by quantitative PCR. Table 1 shows the investigations done during hospital stay. On Day-2 of admission hemi-leminectomy of D6 vertebra followed by biopsy from the involved site was taken by the neurosurgeon.
Table 1: Showing relevant investigations of the patient during hospital stay.
S.No |
Investigation |
Result |
1 |
Hemogram |
Haemoglobin- 162 gm/L, Total leukocyte count 300x109/L, Platelet count- 220 x 109/L |
2 |
Peripheral blood smear |
Red blood cells - normchromic normocytic |
3 |
Bone marrow aspiration and biopsy |
Myeloproliferative neoplasm likely CML with 2% blasts. |
4 |
Quantitative RT PCR for BCR ABL1 |
Major Transcript |
5 |
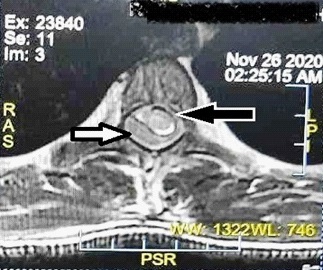
MRI dorsal spine |
Marrow infiltrative disorder with posterior epidural soft tissue component causing compressive myelopathy changes from D2 to L3 (Figure 1,2) |
6 |
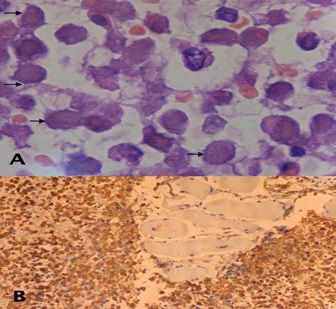
Biopsy |
Shows presence of clusters of blasts along with left shift cells. MPO was strongly positive. (Figure 3) |
Histopathological examination of the biopsy showed presence of myeloid cells including myeloid blasts suggestive of myeloid sarcoma /granulocytic sarcoma.
This 34 years old male presented with paraplegia, sensory loss, very high total leucocyte counts and splenomegaly. The differential diagnosis at presentation was acute leukemia (lymphoid /myeloid), CLL and other lymph proliferative disorders, non hematological malignancy with leukamoid reaction or myeloproliferative neoplasms with extramedullary hematopoieis/ granulocytic sarcoma involving the spinal cord.
At presentation, in view of severe weakness and very high counts he was started on I.V methylprednisolone 30 mg/kg body weight for 3 days followed by prednisolone 1 mg/kg body weight. He was also initiated on cap hydroxyurea 500 mg three times a day for cytoreduction. After confirmation of diagnosis we added Dasatinib 100 mg once a day (Second generation TKI) keeping in view good CNS penetration of this drug and high ELTS score of the patient. Radiotherapy consultation was taken but it was not feasible in view of very long segment of affected spinal cord. Family was counselled regarding poor prognosis. Active physiotherapy was also started. Measures were taken to prevent bed sores. Patient stayed in hospital for 3 weeks. After 1 week of initiation of hydroxyurea his WBC counts reduced to 20 X 109 / L. After 1 week of addition of dasatinib his counts were 4.5 X 109 / L and spleen became non palpable. His power did not improve during these 3 weeks. He was stable at the time of discharge without any improvement in power (0/5) in both lower limbs. Patient was asked to follow up after 2 weeks. He was stable but sensory loss; paraplegia and loss of bladder and bowel control were persistent. The power in his lower limbs was 0/5. He was continued on dasatinib 100 mg OD and was advised regular monthly follow and regular physiotherapy.
In the previous cases spinal cord involvement was confined to a few thoracic vertebrae. In the current case study more extensive spinal cord involvement was noticed and this led to the poor outcome regarding neurological outcome.
Discussion
Malignant Spinal Cord Compression (MSCC) occurs very rarely in cases of chronic myeloid leukemia. Multiple myeloma is the most common cause of malignant cord compression and accounts for 7.9% cases [5]. The presentation of chronic myeloid leukemia in such an acute manner is very uncommon. Most of the cases of chronic myeloid leukemia present with systemic findings and splenomegaly. Very few similar cases are reported in previous literature. Extramedullary tumors or granulocytic sarcomas are seen most frequently in acute myeloid leukemia or CML blast crisis [6].
Apart from the present case there have been five more similar cases which are described in literature. Our case presented with involvement of very long segment of spinal cord extending from D2 to L3. Summary of published cases is given in the Table 2 below.
Table 2: Brief summary of Published cases of CML presenting with cord compression and paraparesis due to granulocitic sarcoma.
References |
Present case |
Ganapule AP et al.[6] |
Barbara J Bryant et al.[7] |
Wildhyde DE et al.[8] |
Rand and Rand et |
Critchley and |
Weil at al.[11] |
Bassoe at al.[12] |
Year of publication |
2021 |
2014 |
2006 |
1963 |
1960 |
1930 |
1935 |
1918 |
Patient age /sex |
34 years male |
43 years /male |
53 years / female |
12 years /female |
6 years/female |
14 years/ male |
39 years /male |
28 years/Female |
Follow up |
ongoing |
- |
4 months |
8 months |
5 months |
4 months |
14 months |
41 months |
Tumor location |
T2 to L3 posterior to the spinal cord |
T6-T8 Paravertebral |
T4-T6 |
T6 |
T1-T5 |
T2, T7 |
T1-T5 |
T4-T6 |
Mechanism of deposition of leukemic cells in spinal cord is not well known. Many times the tumor deposition in spinal cord has a rapid course and is termed as chloroma. It occurs preferentially in subperiosteal region of skull, sternum, ribs and vertebrae [13]. Epidural leukemic involvement may occur at various sites. Rouques et al was of the opinion that the deposition of leukemic cells starts in duramater of spinal cord [14]. Whereas Williams et al suggested the paravertebral lymph node involvement extending into the intervertebral foramina into the epidural space as the reason behind the involvement of spinal canal in leukemia. A third source of involvement of spinal cord is extension from involved vertebrae. Leukemic cells are adhered to the vertebral periosteium or to the superficial layers of the duramater. They are rarely seen infiltrating the pia arachnoid layer hence finding abnormal white blood cells in cerbrospinal fluid is not very common.
In the previous cases spinal cord involvement was confined to a few thoracic vertebrae. In the current case study more extensive spinal cord involvement was noticed and this led to the poor outcome regarding neurological outcome.
References
- Thompson PA, Kantarjian HM, Cortes JE. Diagnosis and Treatment of Chronic Myeloid Leukemia in 2015. Mayo Clin Proc. 2015; 90: 1440-1454.
- Pfirrmann M, Baccarani M, Saussele S, Guilhot J, Cervantes F, Ossenkoppele G, et al. Prognosis of long-term survival considering disease-specific death in patients with chronic myeloid leukemia. Leukemia. 30: 48–56.
- Eser B, Cetin M, Kontas O, Unal A, Er O, Coskun HS, et al. Facial nerve paralysis and paraplegia as presenting symptoms of acute myeloid leukemia. Japanese journal of clinical oncology. 2001; 31: 86-88.
- Mostafavi H, Lennarson PJ, Traynelis VC. Granulocytic sarcoma of the spine. Neurosurgery. 2000; 46: 78-84.
- Loblaw DA, Laperriere NJ, Mackillop WJ. A population-based study of malignant spinal cord compression in Ontario. Clinical Oncology. 2003; 15: 211-217.
- Ganapule AP, Viswabandya A, Jasper A, Patel P, Kokil G. Granulocytic sarcoma with compressive myelopathy: A rare presentation of chronic myelogenous leukemia. Journal of clinical and diagnostic research: JCDR. 2014; 8: QD03.
- Barbara JB, Alperin J, Elghetany MT. Paraplegia as the presenting manifestation of extramedullary megakaryoblastic transformation of previously undiagnosed chronic myeloid leukemia. American Journal of Hematology. 2007; 82: 150-154.
- Wilhyde DE, Jane JA, Mullan S. Spinal epidural leukemia. The American Journal of Medicine. 1963; 34: 281-287.
- Rand RW, Rand CW. Intraspinal Tumors of Childhood. Charles C. Thomas, Springfield. 1960; 111.
- Critchley M, Greenfield JG. Spinal symptoms in chloroma and leukaemia. Brain. 1930; 53: 11-37.
- Weil PE, Bertrand F, Casti M. Les complications medullaries de la leucémie. Sang. 1935; 9: 577.
- Bassoe P. Leukemic infiltration in the spinal canal as a cause of paraplegia. The Journal of Nervous and Mental Disease. 1918; 47: 180-190.
- Kandell EV. Chloroma, review of the literature from 1926-1336. Archives of Internal Medicine. 1937; 59: 691.
- Rouques L. Les complications nerveuses des leucémies. Annals of Medicine. 1946; 47: 152.