
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Discordant GH and IGF-1 levels in a patient with acromegaly and fibrous dysplasia: A case report
Zahra Davoudi1; Yeganeh Farsi2; Seyed Ali Mousavinejad3; Elena Jamali4; Guive Sharifi5*
1 Assistant Professor of Endocrinology, Skull Base Research Center, Loghman Hakim Medical Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2 Student Research Committee, School of Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
3 Assistant Professor of Neurosurgery, Skull Base Research Center, Loghman Hakim Medical Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
4 Department of Pathology, Loghman Hakim Medical Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
5 Professor of Neurosurgery, Skull Base Research Center, Loghman Hakim Medical Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
*Corresponding Author: Guive Sharifi
Professor of Neurosurgery, Skull Base Research
Center, Loghman Hakim Medical Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Email: yeganehfarsi@yahoo.com
Received : Feb 12, 2022
Accepted : Apr 14, 2022
Published : Apr 21, 2022
Archived : www.jcimcr.org
Copyright : © Sharifi G (2022).
Abstract
Introduction: Follow-up management of patients with acromegaly after pituitary surgery is performed by biochemical assessment of Growth Hormone (GH) and Insulin-Like Growth Factor-1 (IGF1). There is increasing recognition of patients who show discordance results between GH and IGF1.
Clinical case: We report on a 38-year-old man with facial and ear pain on the left side. A candidate for canaloplasty, he was referred to our endocrinology clinic because he had symptoms of acromegaly. The clinical suspicion of acromegaly was confirmed using biochemical tests and Magnetic Resonance Imaging (MRI). The patient’s asymmetric facial features and a Computed Tomography (CT) scan of the skull base showed fibrous dysplasia.
After transsphenoidal surgery, the patient’s complaints improved. Hypopituitarism did not occur. The patient’s IGF-1 levels were within the normal range during the postoperative follow-up period. However, the GH levels at baseline and after an Oral Glucose Tolerance Test (OGTT) remained high, which indicated discordant GH and IGF1 levels. Because the patient had normal IGF-1 levels and no clinical signs and symptoms, he was followed up every 3-6 months. The GH and IGF-1 discrepancy persisted for 3 years. After 3 years, the IGF-1 levels increased, which resulted in the patient being treated with longacting octreotide. The patient is currently in remission with medical treatment.
Conclusion: The interpretation of discrepancy between IGF1 level and GH after OGTT in patients with acromegaly during the follow-up requires efficient management of clinical symptoms and biochemical markers in these patients which need close patient-physician cooperation.
Keywords: Growth hormone; Insulin-like growth factor-1; Acromegaly; Fibrous dysplasia.
Citation: Davoudi Z, Farsi Y, Mousavinejad SA, Jamali E, Sharifi G. Discordant GH and IGF-1 levels in a patient with acromegaly and fibrous dysplasia: A case report. J Clin Images Med Case Rep. 2022; 3(4): 1802.
Introduction
Acromegaly is a metabolic disorder that is associated with the production of excessive Growth Hormone (GH) and insulin-like Growth Factor-1 (IGF-1). Patients with acromegaly typically exhibit coarse facial features and acral enlargement [1]. To diagnose acromegaly, GH levels should be measured after an oral glucose tolerance test (OGTT) [1]. Acromegaly can be managed using surgery, medical treatment with somatostatin analogs, and radiotherapy; Transsphenoidal Surgery [TSS] is the preferred treatment [2]. Postoperative concordant levels of GH and IGF-1 are indicators of disease regression, although in some cases, the levels might be discordant [1,3]. The present case report introduced a patient with acromegaly and fibrous dysplasia who had discordant levels of GH and IGF-1 after surgical treatment.
Case presentation
Acromegaly is a metabolic disorder that is associated with the production of excessive Growth Hormone (GH) and insulin-like Growth Factor-1 (IGF-1). Patients with acromegaly typically exhibit coarse facial features and acral enlargement [1]. To diagnose acromegaly, GH levels should be measured after an oral glucose tolerance test (OGTT) [1]. Acromegaly can be managed using surgery, medical treatment with somatostatin analogs, and radiotherapy; Transsphenoidal Surgery [TSS] is the preferred treatment [2]. Postoperative concordant levels of GH and IGF-1 are indicators of disease regression, although in some cases, the levels might be discordant [1,3]. The present case report introduced a patient with acromegaly and fibrous dysplasia who had discordant levels of GH and IGF-1 after surgical treatment.
He did not experience headaches or visual disturbances. The patient noted that the coarse features of acromegaly, such as the enlargement of his nose, lips, and extremities, had occurred after he was 20 years of age. He was married and had two children. The patient complained of excessive sweating and facial pain on the left side.
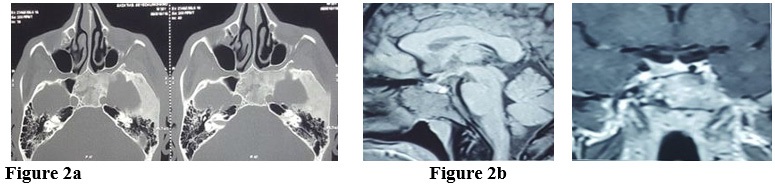
A physical examination revealed that he had symptoms of acromegaly, including acral enlargement, and coarse and asymmetric facial features, which were more prominent on the left side. His height, weight, and blood pressure were 180 cm, 75 kg, and 120/70 mmHg, respectively. In addition to clinical suspicion of acromegaly, his increased levels of IGF-1 (439 ng/mL) led us to administeran OGTT and determine the levels of other pituitary hormones (Table 1). A Magnetic Resonance Imaging (MRI) scan of the pituitary showed that there was amacroadenoma, which measured 12 mm X 10 mm, on the right side of the sella. A Computed Tomography (CT) scan suggested fibrous dysplasia (Figure 2). Thus, we suspected that our patient had comorbid fibrous dysplasia and McCune–Albright syndrome (MAS).
Table 1: Preoperative assessment of pituitary function.
Hormone |
Measured value |
Normal range* |
Units |
||||||
FT4 |
19.6 |
12 _22 |
pmol/L |
||||||
TSH |
0.9 |
0.4_ 4 |
mIU/L |
||||||
PRL |
2.34 |
1.1 - 13 |
ng/mL |
||||||
Cortisol |
12.5 |
520 |
Ug/dL |
||||||
ACTH |
25 |
Up to 48 |
pmol/L |
||||||
LH |
5.5 |
0.7_11 |
IU/L |
||||||
FSH |
3.5 |
0.8_10 |
IU/L |
||||||
Testosterone |
310 |
250_1000 |
ng/dL |
||||||
IGF-1 |
439.8 |
83 – 238 |
ng/mL |
||||||
GH (basal) |
4.5 |
Up to 4 |
ng/mL |
||||||
GH (after an OGTT) |
0 |
30 |
60 |
120 |
0 |
30 |
60 |
120 |
ng/mL |
4.5 |
3.7 |
3.9 |
4.1 |
<1 |
<1 |
<1 |
<1 |
||
* Normal range for a healthy adult young man. FT4: Free Thyroxine; TSH: Thyroid-Stimulating Hormone; PRL: Prolactin; ACTH: Adrenocorticotropic Hormone; LH: Luteinizing Hormone; FSH: Follicle-Stimulating Hormone; IGF-1: Insulin-Like Growth Factor-1; Andgh: Growth Hormone.
The patient underwent TSS. A pathologic examination of the mass was compatible with a pituitary adenoma. Table 2 shows the immuno cytochemical analysis of the pituitary adenoma.
Table 2: Immunocytochemical analysis of pituitary adenoma.
Tumor marker |
% of presence |
Ki-67 |
2-3 % |
P-53 |
6% (weakly positive) |
GH |
Positive (densely granulated) |
PRL |
Negative |
After surgery, the patient’s complaints improved. Hypopituitarism did not occur in the patient. Although the IGF-1 levels were within the normal range during the postoperative follow-up period, the GH levels at baseline and after an OGTT remained high, which indicated that the patient had discordant GH and IGF-1 levels (Table 3). Subsequent MRI scans showed normal findings in the radiology report. Due to the normal levels of IGF-1 and the absence of any clinical signs and symptoms, we measured the GH levels every 2 hours from 8 AM until 8 PM and determined that the mean GH level was 2.7 ng/mL.
Table 3: IGF-1 and GH Levels during Follow-Up.
Hormone (units) |
3 months after surgery |
6 months after surgery |
12 months after surgery |
3 years after surgery |
3–6 months after medical treatment |
IGF-1(ng/mL) |
179 |
182 |
170 |
267 |
170 |
GH (ng/mL) |
3.0 |
3.7 |
2.8 |
3.76 |
0.8 |
The patient was followed up every 3-6 months. The discordant GH and IGF-1 levels were sustained for 3 years. After 3 years, there was an increase in the IGF-1 and GH levels: 267 ng/ mL and 3.76 ng/mL, respectively. The patient was given medical treatment with long-acting octreotide monthly. The patient is currently in remission with medical treatment.
Serum IGF-I was measured through the chemiluminescence Immunoassay Immunodiagnostic Systems (IDS-iSYS, IDS Nordic A/S). Analyses showed the Coefficient of Variation (CV) to be 7.2%, at 304 ng/ml. The age- and gender-adjusted levels of IGFI were also expressed as IGFI×upper limit of the normal (IGFI×ULN). Consequently, calibrators of this kit were traceable to the World Health Organization (WHO) international standard for IGF-I, code 02/254, with a reportable range of 10 to 1200 ng/ml. Serum GH levels were measured through chemiluminescence immunoassay with the use of Cobas E601 analyzer (Roche Diagnostics, Indianapolis, Indiana: USA) considering a lower LOD for GH equal to 0.03 ng/ml and assay linearity ranged between 0.03 and 50.0 ng/ml.

Discussion
Our patient had features of acromegaly and excess GH; the CT scans were compatible with fibrous dysplasia. The patient was diagnosed with comorbid fibrous dysplasia/MAS [4,5]. However, our patient had no café-au-lait spots, which have been described in other case reports [6-8]. Genetic testing would definite the diagnosis but it was not appliable for us to perform it.
Salenave et al. reviewed 112 patients with MAS and acromegaly; only 25 patients underwent surgery [9]. Therapeutic strategies for acromegaly in patients with MAS are almost identical to those for patients with classic acromegaly. However, it can be difficult to perform pituitary surgery in patients with MAS because of the thickness of cranial dysplasia at the base of the skull, especially when the sphenoid bone is involved [9]. Our patient underwent TSS.
GH and IGF-1 levels are not only used to diagnose acromegaly, but they are also markers of remission/recurrence during follow-up [1,6-8]. In 2000, a group developed a consensus statement about postoperative indicators for the control of acromegaly, which included normal IGF-1 levels and the lowest GH level (˂1 μg/L) after an OGTT using 75 g glucose [10]; while new consensus guidelines recommend normal IGF1 level and GH random (GHr) of less than ng/mL and a GH nadir (GHn) of less than 0.4 l ng/mL in OGTT [11].
The goals of surgery in acromegaly are not only to normalize IGF1 and GH levels but also to improve clinical symptoms and signs and Quality of Life (QoL) [12].
In addition, because IGF-1 and GH are concordant in most patients, decreased levels indicate remission of acromegaly, while increased levels suggest active disease [1,13]. Based on the current literature, 25% of patients exhibit discordant IGF-1 and GH levels after treatment; this discrepancy can be attributed to underlying diseases or differences in measurement techniques or cut-off values [3,13,14].
Freda et al. found that when patients had normal IGF-1 levels, an abnormal OGTT could potentially be a marker for predicting subsequent biochemical relapse; this occurred in our patient [15]. Both Sheppard and Freda et al. observed that patients with acromegaly who had discordant levels after undergoing TSS had an increased risk of disease recurrence [15,16]. However, this finding has not been confirmed in other reports. Other studies found that there was no gradual increase in GH and/or IGF-1 levels during a 2–5-year follow-up of patients with persistent discordant levels [17,18]. Increased IGF-1 and GH levels might be observed due to the neural dysregulation of GH [15]. Thus, it is necessary to monitor the risk of active disease recurrence [15,18].
Similar to Kaltsas et al., we assessed the GH levels of our patient throughout the day [19]. Although this method is more accurate than taking a single measurement, it has a higher cost and may not be acceptable for all patients.
During the follow-up, we monitored our patient for clinical and laboratory findings and MRI every 3 to 6 months that did not change significantly; until IGF-1 levels rose within three years and medical therapy was initiated, given that this patient with fibrous dysplasia was not a candidate for reoperation or radiotherapy.
According to the stepwise approach and management of these patients, proposed by M. Zeinalizadeh et al. and Freda et al. in cases with mean diurnal GH of more than 1 ug/l, in the absence of clinical symptoms and signs, close clinical follow-up and biochemical evaluation every 3–6 months is justified [15,20].
Many of these patients have no tumor remnant on imaging studies, a second transsphenoidal surgery is not logical.
In such a situation, additional treatments such as pharmacological medications should be individualized.
Conclusion
In conclusion, the interpretation of discrepancy between IGF1 level and GH after OGTT in patients with acromegaly during the follow-up requires efficient management of clinical symptoms and biochemical markers in these patients which need close patient-physician cooperation.
Declarations
Ethical issues: A voluntary consent form was obtained from the patient.
Ethical issues: A voluntary consent form was obtained from the patient.
Acknowledgments: The authors express their appreciation to the Skull-Base Research Center (SBRC), Loghman Hakim Hospital, which is affiliated with the Shahid Beheshti University of Medical Sciences, Tehran, Iran, for supporting and assisting with the implementation of this case report.
References
- Akirov A, Masri Iraqi H, Dotan I, Shimon I. The Biochemical Diagnosis of Acromegaly. Journal of clinical medicine. 2021; 10.
- Giustina A, Barkhoudarian G, Beckers A, Ben-Shlomo A, Biermasz N, Biller B, et al. Multidisciplinary management of acromegaly: A consensus. Rev Endocr Metab Disord. 2020; 21: 667- 678.
- Campana C, Cocchiara F, Corica G, Nista F, Arvigo M, Amarù J, et al. Discordant GH and IGF-1 Results in Treated Acromegaly: Impact of GH Cutoffs and Mean Values Assessment. The Journal of clinical endocrinology and metabolism. 2021; 106: 789-801.
- Holbrook L, Brady R. McCune Albright Syndrome. StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2021, StatPearls Publishing LLC.; 2021.
- Javaid MK, Boyce A, Appelman-Dijkstra N, Ong J, Defabianis P, Offiah A, et al. Best practice management guidelines for fibrous dysplasia/McCune-Albright syndrome: A consensus statement from the FD/MAS international consortium. Orphanet J Rare Dis. 2019; 14: 139.
- Natarajan MS, Prabhu K, Chacko G, Rajaratnam S, Chacko AG. Endoscopic transsphenoidal excision of a GH-PRL-secreting pituitary macroadenoma in a patient with McCune-Albright syndrome. British journal of neurosurgery. 2012; 26: 104-106.
- Classen CF, Mix M, Kyank U, Hauenstein C, Haffner D. Pamidronic acid and cabergoline as effective long-term therapy in a 12-yearold girl with extended facial polyostotic fibrous dysplasia, prolactinoma and acromegaly in McCune-Albright syndrome: A case report. Journal of Medical Case Reports. 2012; 6: 32.
- Bhadada SK, Bhansali A, Das S, Singh R, Sen R, Agarwal A, et al. Fibrous dysplasia & McCune-Albright syndrome: An experience from a tertiary care centre in north India. The Indian journal of medical research. 2011; 133: 504-509.
- Salenave S, Boyce AM, Collins MT, Chanson P. Acromegaly and Mc Cune-Albright syndrome. The Journal of clinical endocrinology and metabolism. 2014; 99: 1955-1969.
- Giustina A, Barkan A, Casanueva FF, Cavagnini F, Frohman L, Ho K, et al. Criteria for cure of acromegaly: A consensus statement. The Journal of clinical endocrinology and metabolism. 2000; 85: 526-529.
- Giustina A, Chanson P, Bronstein MD, Klibanski A, Lamberts S, Casanueva FF, et al. A consensus on criteria for cure of acromegaly. The Journal of clinical endocrinology and metabolism. 2010; 95: 3141-3148.
- Neggers SJ, Biermasz NR, van der Lely AJ. What is active acromegaly and which parameters do we have? Clinical endocrinology. 2012; 76: 609-614.
- Kanakis GA, Chrisoulidou A, Bargiota A, Efstathiadou ZA, Papanastasiou L, Theodoropoulou A, et al. The ongoing challenge of discrepant growth hormone and insulin-like growth factor I results in the evaluation of treated acromegalic patients: A systematic review and meta-analysis. Clinical endocrinology. 2016; 85: 681-688.
- Schilbach K, Strasburger CJ, Bidlingmaier M. Biochemical investigations in diagnosis and follow up of acromegaly. Pituitary. 2017; 20: 33-45.
- Freda PU, Nuruzzaman AT, Reyes CM, Sundeen RE, Post KD, et al. Significance of “abnormal” nadir growth hormone levels after oral glucose in postoperative patients with acromegaly in remission with normal insulin-like growth factor-I levels. The Journal of clinical endocrinology and metabolism. 2004; 89: 495-500.
- Sheppard MC. GH and mortality in acromegaly. Journal of endocrinological investigation. 2005; 28: 75-77.
- Ronchi CL, Varca V, Giavoli C, Epaminonda P, Beck-Peccoz P, Spada A, et al. Long-term evaluation of postoperative acromegalic patients in remission with previous and newly proposed criteria. The Journal of clinical endocrinology and metabolism. 2005; 90: 1377-1382.
- Ronchi CL, Arosio M, Rizzo E, Lania AG, Beck-Peccoz P, et al. Adequacy of current postglucose GH nadir limit (< 1 µg/l) to define long-lasting remission of acromegalic disease. Clinical endocrinology. 2007; 66: 538-542.
- Kaltsas GA, Isidori AM, Florakis D, Trainer PJ, Camacho-Hubner C, et al. Predictors of the outcome of surgical treatment in acromegaly and the value of the mean growth hormone day curve in assessing postoperative disease activity. The Journal of clinical endocrinology and metabolism. 2001; 86: 1645-1652.
- Zeinalizadeh M, Habibi Z, Fernandez-Miranda JC, Gardner PA, Hodak SP, et al. Discordance between growth hormone and insulin-like growth factor-1 after pituitary surgery for acromegaly: A stepwise approach and management. Pituitary. 2015; 18: 48- 59.