
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Air on the brain: Cerebral embolism associated with outpatient line
Aaron Lee Haag
Allegheny Health Network, Pittsburgh, PA, USA
*Corresponding Author: Aaron Lee Haag
Allegheny Health Network, Pittsburgh, PA, USA
Email: Aaron.Haag@ahn.org
Received : Mar 28, 2022
Accepted : Apr 18, 2022
Published : Apr 25, 2022
Archived : www.jcimcr.org
Copyright : © Haag AE (2022).
Citation: Haag AE. Air on the brain: Cerebral embolism associated with outpatient line. J Clin Images Med Case Rep. 2022; 3(4): 1806.
Introduction
We present a case of a 64-year-old male with a patent foramen ovale who suffered severe complications from a massive air embolism while accessing a tunneled CVC. Air embolism may occur in conjunction with trauma, diving accidents, hemodialysis, cardiopulmonary bypass surgery, neurosurgery, thoracic biopsies, or transpulmonary passage from barotrauma, but it is most often associated with central venous catheter (CVC) insertions [1]. Arterial air embolisms, particularly cerebral air embolisms, are a rare and potentially fatal event that may result in severe, irreversible neurological deficits [2]. High index of suspicion is necessary, especially in those with an underlying cardiac defect such as a patent foramen ovale (PFO), where a paradoxical embolism may occur. With an underlying PFO, a baseline left to right shunt may undergo reversal of the shunt due to a raise in the right atrial pressures, mostly associated with Valsalva, and thus result in cerebral arterial embolism [1,3].
Case presentation
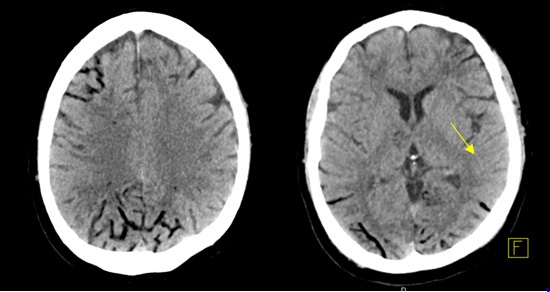
64-year-old male with a history of prostate adenocarcinoma, pulmonary embolism on anticoagulation, and multiple myeloma was originally admitted to the hospital to undergo a stem cell transplant. A tunneled chest port (right subclavian CVC), which was placed 14 days prior, was accessed for routine lab work prior to transplant. Immediately after this attempt, patient was found unresponsive. His physical exam revealed asymmetric pupils without response to noxious stimuli. CT Head showed extensive foci of bilateral sulcal hypoattenuation concerning for air embolism along with multiple areas of evolving infarct (Figure 1). Magnetic resonance imaging (MRI) revealed diffuse areas of sulcal FLAIR signal abnormalities, again concerning for air embolism. Subsequently, an echocardiogram showed evidence of right to left shunting from a PFO. Patient was then transferred to the Intensive Care Unit (ICU) for acute neurologic dysfunction. He required emergent intubation for airway protection.
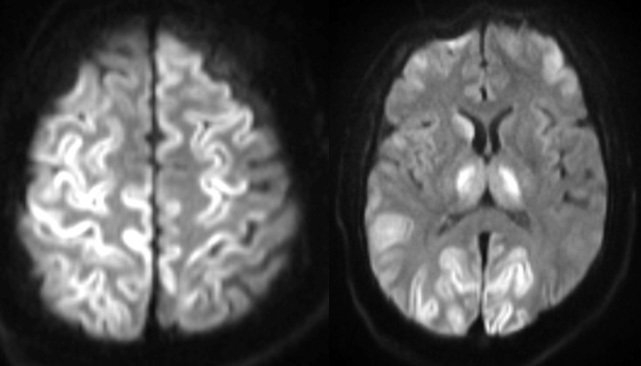
As part of further management, the patient was transferred to a facility with a hyperbaric oxygen (HBO) chamber. During his initial HBO therapy, which was initiated after only 12 hrs from the time of unresponsiveness, the patient was noted to have seizure like activity and the target pressure was unfortunately never achieved. Prompt initiation of levetiracetam, uptitration of the ongoing propofol infusion, and the addition of a midazolam infusion was administered for seizure management. Persistence of seizure like activity in the HBO chamber despite antiepileptic agents warranted aborting the therapy for time-sensitive medical management. An electroencephalogram (EEG) revealed severe cerebral dysfunction without any active epileptiform activity. This seizure like activity was then deemed to be clinical myoclonic status epilepticus. With persistence of status myoclonus and no improvement in neurological exam, a repeat MRI was performed that showed severe hypoxic injury and edema involving both cerebral cortexes diffusely, the thalami, and right caudate nucleus (Figure 2). Family ultimately transitioned him to comfort care measures only.
Discussion
We present a case of paradoxical embolism associated with a patent foramen ovale which occurred while accessing a CVC resulting in cerebral air embolism. The subsequent delay in hyperbaric oxygen therapy led to anoxic brain injury causing severe, irreversible neurological deficits.
Following initial evaluation to rule out an acute stroke, most of the management for air embolism is primarily supportive in nature [4]. However, HBO therapy must be considered if a patient is noted to have developed i) acute neurological dysfunction ii) shock from cardiopulmonary compromise, or iii) other organ ischemia [4]. The mechanism by which HBO can potentially reverse these catastrophic consequences is unclear, however the potential favorable impact may be due to mechanical reduction of the size of the air bubbles through the absorption of nitrogen from the gas bubble, further alleviating local tissue hypoxia. This accepted therapy for cerebral air embolism, has a “golden hour” and patients who receive it within the critical 4-6 hrs from the occurrence of the event have the greatest opportunity to benefit from therapy [5,6]. Hyperbaric therapy itself rarely reduces the seizure threshold, however the risk of seizures may be increased as the neurologic deficits progress, leading to an interruption in the definitive therapy, like in our patient [7,8]. Thus, there are several barriers to initiation of hyperbaric therapy including patient stability prior to receiving the HBO therapy, patient’s access to HBO facility, and health care provider awareness of this golden hour to get to the HBO facility [6,9-11].
Our case highlights the delay in timely diagnosis and recognition of severity, the substantial gap in the knowledge of targeting this golden hour for hyperbaric therapy, the consequent delay in referral to hyperbaric facility, and the heightened risk of complications like seizures from delayed initiation of hyperbaric therapy itself, all of which culminated into an unfortunate outcome with anoxic brain injury. Hence, following immediate resuscitative efforts, we emphasize the importance of educating health care providers to initiate the referral process emergently, as one would for a patient with an ischemic stroke, in an effort to initiate therapy within the “golden hour”. This would help overcome one of critical barriers of pursuing time sensitive efforts with hyperbaric therapy that may completely reverse and prevent lethal complications associated with cerebral air embolism.
Conclusions
A strong emphasis must be placed on educating health care providers caring for or inserting CVCs to prevent complications such as air embolisms. In cases where suspicion of an air embolism arises, especially in those associated with neurologic dysfunction, urgent referral to a facility within the golden hour to attain hyperbaric therapy is critical to achieve favorable outcomes.
References
- Kerrigan MJ, Cooper JS. Venous Gas Embolism. [Updated 2021 Oct 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih. gov/books/NBK482249/
- Carneiro AC, Diaz P, Vieira M, Silva M, Silva I, Custodio M, Faria M. Cerebral Venous Air Embolism: A Rare Phenomenon. Eur J Case Rep Intern Med. 2019; 6(1): 001011. doi: 10.12890/2019_001011. PMID: 30756075; PMCID: PMC6372048.
- Hakman EN, Cowling KM. Paradoxical Embolism. [Updated 2021 Sep 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. 2022. Available from: https://www.ncbi.nlm.nih. gov/books/NBK470196/
- Gordy S, Rowell S. Vascular air embolism. Int J Crit Illn Inj Sci. 2013; 3(1): 73-76. doi:10.4103/2229-5151.109428.
- Leitch DR, Green RD. Pulmonary barotrauma in divers and the treatment of cerebral arterial gas embolism. Aviat Space Environ Med. 1986; 57(10 Pt 1): 931-8. PMID: 3778391.
- Blanc P, Boussuges A, Henriette K, Sainty JM, Deleflie M. Iatrogenic cerebral air embolism: importance of an early hyperbaric oxygenation. Intensive Care Med. 2002; 28(5): 559-63. doi: 10.1007/s00134-002-1255-0. Epub 2002 Mar 21. PMID: 12029402.
- Hadanny A, Meir O, Bechor Y, Fishlev G, Bergan J, Efrati S. Seizures during hyperbaric oxygen therapy: retrospective analysis of 62,614 treatment sessions. Undersea Hyperb Med. 2016; 43(1): 21-8. PMID: 27000010.
- Muller Fenna F, van Hulst, Robert A, Coutinho Jonathan M, Weenink Robert P. Seizures in Iatrogenic Cerebral Arterial Gas Embolism, Critical Care Explorations. 2021; 3(8): e0513. doi: 10.1097/CCE.0000000000000513.
- Mirski MA, Lele AV, Fitzsimmons L, Toung TJ. Diagnosis and treatment of vascular air embolism. Anesthesiology. 2007; 106(1): 164-77. doi: 10.1097/00000542-200701000-00026. PMID: 17197859.
- Lattin G Jr, O’Brien W Sr, McCrary B, Kearney P, Gover D. Massive systemic air embolism treated with hyperbaric oxygen therapy following CT-guided transthoracic needle biopsy of a pulmonary nodule. J Vasc Interv Radiol. 2006; 17(8): 1355-8. doi: 10.1097/01.RVI.0000231949.35479.89. PMID: 16923984.
- Wherrett CG, Mehran RJ, Beaulieu MA. Cerebral arterial gas embolism following diagnostic bronchoscopy: delayed treatment with hyperbaric oxygen. Can J Anaesth. 2002; 49(1): 96-9. doi: 10.1007/BF03020427. PMID: 11782337.