
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Von Recklinghausen disease revealed by breast node: Case report
S Fekkoul*; O Lamzouri; H Taheri; H Saadi; A Mimouni
Department of Obstetrics and Gynecology, Mohammed VI University Hospital Center, Oujda, Morocco.
*Corresponding Author: Soukaina Fekkoul
Department of Obstetrics and Gynecology, Mohammed VI University Hospital Center, Oujda, Morocco.
Email: soukaynafek@gmail.com
Received : Mar 24, 2022
Accepted : Apr 19, 2022
Published : Apr 26, 2022
Archived : www.jcimcr.org
Copyright : © Fekkoul S (2022).
Abstract
Neurofibromatosis causes various types of benign or malignant tumors of the central or peripheral nerves and often causes pigmented macules of the skin and sometimes other manifestations. We present a case of 29 years old patient diagnosed by neurofibromatosis manifested by breast lesion, at the beginning, the diagnosis was not clear, but after the anatomopalogist report von Recklinghausen disease was suspected and the patient was having all the criteria to confirm that. Recent scientific data support a possible association between breast cancer and NF1. It has been suggested that there may be genes that could interact with the NF1 gene, particularly in relation to the BRCA1 subset. They could share a common gene location (both NF1 and BRCA1 are on human chromosome 17q). Multiple cutaneous lesions in NF-1 may obscure breast lumps leading to delayed detection of cancer. Early onset, aggressive behavior and different natural history of these tumors require a specific approach to their detection and management.
Keywords: Breast; Neurofibromatosis; Von Recklinghausen disease; Neurofibromas; Café au lait spots; Neurofibromin; nf1 gene; b and 17q11.2.
Citation: S Fekkoul, O Lamzouri, H Taheri, H Saadi, A Mimouni. Von Recklinghausen disease revealed by breast node: Case report. J Clin Images Med Case Rep. 2022; 3(4): 1808.
Introduction
Neurofibromatosis is a group of interrelated disorders with overlapping clinical manifestations that are now known to have distinct genetic causes. It causes various types of benign or malignant tumors of the central or peripheral nerves and often causes pigmented macules of the skin and sometimes other manifestations. The diagnosis is clinical. There is no specific treatment, but benign tumors can be surgically removed, and malignant tumors (which are less common) can be treated with radiation or chemotherapy. We present a case of a 29 years old patient who presented a breast tumor that revealed a type 1 neurofibromatosis.
Case report
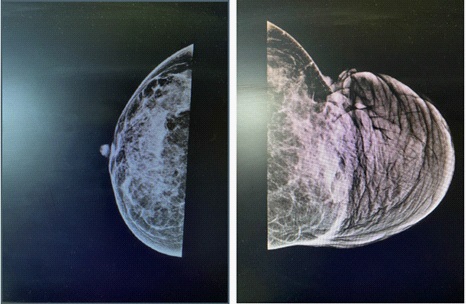
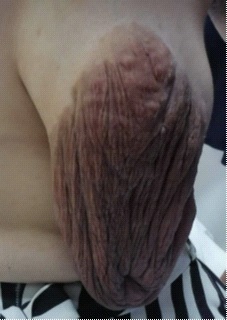
Mrs. K.A., 29 years old, married, mother of three living children, with no personal history presented for mastodynia with hypertrophy of the areolar plate. The clinical examination on admission showed a hemodynamically stable patient, on senological examination an hypertrophy of the areolar plate of the left breast measuring 8 cm with externally deviated nipple, with no inflammatory signs, no palpable nodule (Figure 3). The right breast was without abnormalities. There were no associated axillary or supra-clavicular adenopathies. Several café au lait spots were visible on all the teguments, the smallest measured 20 mm in diameter. Echo-mammography: breast classified as BIRADS 2, hypertrophy of the skin tissue of the areolar plate of homogeneous hyperechogenic technostructure crossed by thin-walled fusiform galactophoric ducts measuring 16 mm. (Figure 2). A skin biopsy of the breast was performed with immunohistochemical study, followed by resection of the areolar plaque of the breast. The skin biopsy of the breast and the specimens, taken from the areola-nipple plate resection, were fixed in 10% buffered formalin, embedded in kerosene and stained with hematinic-eosin. Complementary immunostaining with antibodies, anti-vimentin (mesenchymal cell marker), antiproteine-S100 (PS100, nerve cell marker), anti-smooth muscle actin (SMA) and anti desmin (both muscle tissue markers) was performed using the peroxide anti-peroxidase method.
Resection of the areola-nipple plate of the breast: At exploration of the breast a mass causing its ptosis with position of the patient’s nipple, incision around the nipple keeping an infero external pedicle, reduction of the tumor with repositioning of the nipple in symmetry with the contralateral nipple (Figure 1). The histological aspect of the skin biopsy of the breast showed an epidermal layer of regular thickness without cytonuclear atypia resting on a dermis with a poorly limited, moderately cellular tumor proliferation made of wavy spindle cells with a regular nucleus and a pale cytoplasm without cytonuclear atypia and without mitoses. These cells are arranged within a fibrillar stroma with numerous capillaries and mast cells. At the level of the tumor proliferation, we note the presence of very rare regular nerve structures.
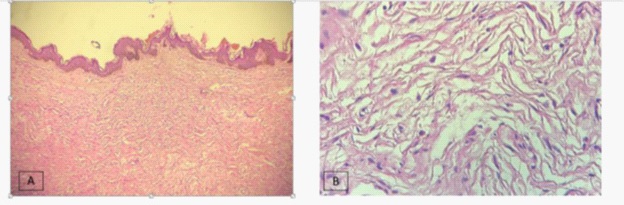
A complementary immunohistochemical study showed that the tumor cells expressed the PS100 protein confirming the histological diagnosis of neurofibroma with no histological signs of malignancy. The resection specimen of the nipple-areolar plate measured 21 X 15 X 3.5 cm. On section, there was a homogeneous nodular whitish lesion with a soft consistency, measuring 9.5 X 6 X 2 cm. It is located 0.4 cm from the deep border. Histologically, it is a cutaneous tissue covered by a regular squamous epithelium. The dermis is the site of a benign, poorly restricted tumor proliferation consisting of spindle-shaped, wavy cells with elongated nuclei and pale cytoplasm. The stroma is finely fibrillated, with some congestive capillaries and mononuclear inflammatory cells. Absence of cytonuclear atypia or mitoses. The tumor is located within 1 mm of the deep border, and in contact with the nearest lateral border (Figure 1). These results allowed us to conclude and retain the diagnosis of a plexiform neurofibroma with diffuse breast localization.
A Von Recklinghausen disease was confirmed in view of the presence of café au lait stains and the presence of plexiform neurofibroma. Peripheral nerve sheath tumors, rhabdomyosarcoma, phaeochromocytoma, somatostatin-producing carcinoid tumors of the duodenal wall, medullary thyroid cancer, and hypothalamic or optic nerve tumors tests were negative. The patient was transferred to genetics department.
Discussion
Neurofibromatosis is a neurocutaneous syndrome (a syndrome with neurological and skin manifestations). There are several types of neurofibromatosis. Neurofibromatosis type 1 (NF1, or von Recklinghausen disease) is the most common, occurring in 1 in 2500 to 3000 subjects. It causes neurological, cutaneous and sometimes orthopedic manifestations. The NF1 gene is located on band 17q11.2 and codes for the synthesis of neurofibromin >1000 mutations have been identified. Although it is an autosomal dominant disorder, 20-50% of cases are caused by isolated germ cell mutation. Neurofibromatosis type 2 (NF2) accounts for 10% of cases and occurs in approximately 1 in 35,000 individuals. It manifests itself mainly as bilateral congenital acoustic neuromas (vestibular schwannomas). The NF2 gene is located on band 22q11 and encodes Merlin, a tumor suppressor; 200 mutations have been identified. Most people with NF2 have inherited it from one of their parents. Schwannomatosis, a rare disease, is classified as a 3rd type of neurofibromatosis. In 15% of cases, this type is familial and is linked to a germline mutation in the SMARCB1 gene, a tumor suppressor gene located on 22q11.23, which is very close to the NF2 gene. In the other cases, the genetic basis is not well understood, but in the tissues of some patients, other mutations of the same gene are involved.
Neurofibromatosis type-1 is an autosomal dominant genetic disorder, mainly caused by mutations of the NF1 gene, which is located on chromosome 17q11 [4,5]. The NF-1 gene is a large tumor suppressor gene that encodes the 327-d protein known as neurofibromin. The predominant features of the disease are benign cutaneous neurofibromas and cafe-au-lait spots. The overall risk of cancer is 4 to 5 times higher than the general population [4]. Frequently associated cancers are malignant peripheral nerve sheath tumors, rhabdomyosarcoma, phaeochromocytoma, somatostatin-producing carcinoid tumors of the duodenal wall, medullary thyroid cancer, and hypothalamic or optic nerve tumors that cause precocious puberty. Majority of the tumors are from connective tissue, endocrine glands and brain parts. But, NF-1 association with breast cancer remains uncommon. Interestingly, these tumors behave in a different manner and have a different natural history from those occurring sporadically. Majority of the breast cancer patients are not only young but also present their disease at an advanced stage with more negative prognostic factors.
In a review of 37 cases of breast cancer associated with NF1, Murayama et al. [6] found that most of the cases had lesions greater than T2 (advanced stage) with invasive duct carcinoma histology. They conclude that the late stage presentation was probably because of the presence of numerous skin neurofibromas that has hindered the discovery of the breast lumps.
In a Japanese review, Nakamura et al. [7] found that in 18.5 % of the cases of NF1, the breast cancer patients were younger than 35 years old. Two recent series have shown a significantly higher risk of developing breast cancer in women with NF-1 younger than 50 years of age. Recent scientific data support a possible association between breast cancer and NF1. It has been suggested that there may be genes that could interact with the NF1 gene, particularly in relation to the BRCA1 subset. They could share a common gene location (both NF1 and BRCA1 are on human chromosome 17q) [5]. Ceccaroni et al. [5] observed five members of a family affected by both NF1 and breast or ovarian cancer, and they showed that three individuals shared a common haplotype, including the NF1 and BRCA1 loci on chromosome 17 and a BRCA1 mutation. They concluded that the concurrence of NF1 and hereditary breast or ovarian cancer in the family was likely because of the two linked mutations at the NF1 and BRCA1 loci.
Veronesi et al. [8] in a study of familial breast cancer showed that BRCA1-positive patients tended to be more often premenopausal, and they had more frequently negative prognostic factors. Similarly, most cases of breast cancer in NF1 occur in women aged less than 50 years [9]. Similar to these published reports, we also observed that our patient had advanced disease at young age.
Conclusion
Breast cancer occurrence in the background of NF-1 is a rare phenomenon. Multiple cutaneous lesions in NF-1 may obscure breast lumps leading to delayed detection of cancer. Early onset, aggressive behavior and different natural history of these tumors require a specific approach to their detection and management. Increasing awareness of this rare possibility needs to be transferred to the patients and treating doctor both, to pickup more and more tumors at a very early stage.
References
- Kumar K, Abbas AK, Fausto N. Neoplasia.In: Robbins and Cotran Pathologic Basis of Disease.7th Ed. Philadelphia: WB Saunders. 2004; 305
- Walker L, Thomson D, Easton D, et al. A prospective study of Neurofibromatosis type1 cancer incidence in the UK. Br J Cancer. 2006; 195: 233-238. doi: 10.1038/sj.bjc.6603227.
- Roberta I, Barbara M, Graziella P. Association of GIST, breast cancer and Schwannoma in a 60- year old woman affected by type1 von Recklinghausen’s neurofibromatosis. Tumori. 2008; 194: 126-128.
- Zoller ME, Rembeck B, Oden A, Samuelsson M, Angervall L. Malignant and benign tumors in patients with neurofibromatosis type 1 in a defined Swedish population. Cancer. 1997; 79: 2125-2131. doi: 10.1002/(SICI)1097-0142(19970601)79:11<2125::AIDCNCR9>3.0.CO;2-N.
- Ceccaroni M, Genuardi M, Legge F, Lucci-Cordisco E, Carrara S, D’Amico F, et al. BRCA1-related malignancies in a family presenting with von Recklinghausen’s disease. Gynecol Oncol. 2002; 86: 375-378. doi: 10.1006/gyno.2002.6757.
- Murayama Y, Yamamoto Y, Shimojima N, Takahara T, Kikuchi K, Iida S, et al. T1 breast cancer associated with von Recklinghausen’s neurofibromatosis. Breast Cancer. 1999; 6: 227-230. doi: 10.1007/BF02967173.
- Nakamura M, Tangoku A, Kusanagi H, Oka M, Suzuki T. Breast cancer associated with Recklinghausen’s disease: report of a case. Nippon Geka Hokan. 1998; 67: 3-9.
- Veronesi A, de Giacomi C, Magri MD, Lombardi D, Zanetti M, Scuderi C, et al. Familial breast cancer: characteristics and outcome of BRCA 1–2 positive and negative cases. BMC Cancer. 2005; 5: 70. doi: 10.1186/1471-2407-5-70.
- Sharif S, Moran A, Huson SM, Iddenden R, Shenton A, Howard E, et al. Women with neurofibromatosis 1 are at a moderately increased risk of developing breast cancer and should be considered for early screening. J Med Genet. 2007; 44: 481-484. doi: 10.1136/jmg.2007.049346.