
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Shot gun eye injuries: Senegalese experience
Jean Pierre Diagne*; Aly MbaraKa; Alassane Ba; Yassine R; M EQ De Meideros; P A Ndiaye
Cité Universitaire Fann Hock Campus A 2-1-8 DAkar/Sénégal.
*Corresponding Author: Jean Pierre Diagne
DCité Universitaire Fann Hock Campus A 2-1-8
DAkar/Sénégal.
Email: sebanemack@yahoo.fr
Received : Feb 15, 2022
Accepted : Apr 20, 2022
Published : Apr 27, 2022
Archived : www.jcimcr.org
Copyright : © Diagne JP (2022).
Abstract
Purpose: To describe the cases of eye trauma caused by the use of home-made firearms and to highlight the difficulties of their management.
Observations: We admitted five patients (0.16%) with firearm-related eye injuries during the period from January 01, 2010 to January 01, 2022. All our patients were male. The average age was 33.2 years with extremes between 21 and 55 years. The circumstances of occurrence were dominated by attacks with lead as the main traumatic agent in all our patients. The consultation time ranged from one week to three months with a starting visual acuity not exceeding the light perception. The lesions were bilateral in three patients. There was a loss of eyeball function in all patients. Intraocular foreign bodies were found in 80% of cases. All our patients received medical treatment. Two of our patients had received surgical treatment such as extra capsular extraction and anterior vitrectomy.
Discussion and conclusion: Shot-gun eye injuries have increased in recent years. Facial screening makes all the severity of these traumas involving the functional prognosis of the eye. Young people in full employment are mainly affected, hence the importance of prevention.
Keywords: Eye; Shot weapons; Trauma; Prognosis; Prevention.
Citation: Diagne JP, Mbaraka A, Yassine R, De Meidero ME, Ndiaye PA. Shot gun eye injuries: Senegalese experience. J Clin Images Med Case Rep. 2022; 3(4): 1809.
Introduction
Gunshot eye injuries are the most common type of gun injury. They are a major therapeutic emergency. These traumas are of forensic interest. CT head and B-scan ocular ultrasound allow the localization of different shot sizes. These weapons are classified in the 4th category of firearms and are therefore prohibited by law. The shooting is done in cone, responsible for a scattering in sheaf of shot. These pellets are made of pellets containing impurities. They are designed not to be “dangerous” and are stopped by the bone, but they cause lesions of the soft parts whose severity and bilaterality depend on several parameters [1]. The vulnerability of a projectile depends on its energy its shape, its stability, the density and elasticity of the tissues traversed [2]. Hence the severity of the lesions if the projectiles reach the eyes. Facial screening does all the functional gravity of these weapons because of the visual prognosis that is involved by almost constant impairment of one or both eyes [3].
The purpose of our study was to describe cases of ocular trauma caused by the use of home-made firearms and to highlight the difficulties of their management.
Observations
We had received in our center, over a period of 12 years from January 01, 2010 to January 01, 2022, five patients for eye trauma with shot weapons. They received a complete ophthalmological examination, a neurosurgical opinion and a lesion assessment including a CT head (orbits and brain), a B-scan ocular ultrasound (10 MHz probe) and a standard x-ray of the bones of the nose. The Ocular Trauma Score (OTS) [4] was evaluated for 4 patients, one patient having seen three months after the trauma; we did not have his initial visual acuity. The extraction of the granules in subcutaneous and cutaneous was performed in all patients.
Case Series
Case 1
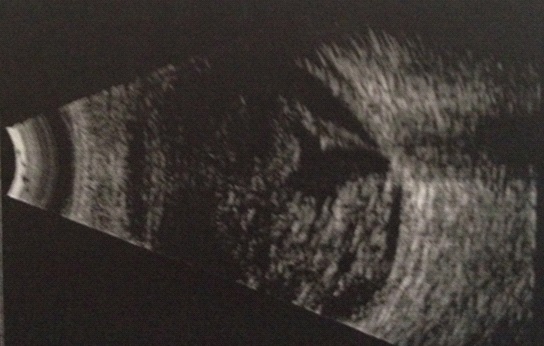
This was a 22-year-old patient who was referred for the management of bilateral intravitreal hemorrhage following a blast from an attack a week earlier. Visual Acuity (VA) was reduced to a Light Perception (LP+) in both eyes. At biomicroscope, the lesions were bilateral marked by: Diffuse Subconjunctival Hemorrhage (SCH), hypotonia, post-traumatic cataract, medium-density Vitreous Hemorrhage (VH) and total retinal detachment.
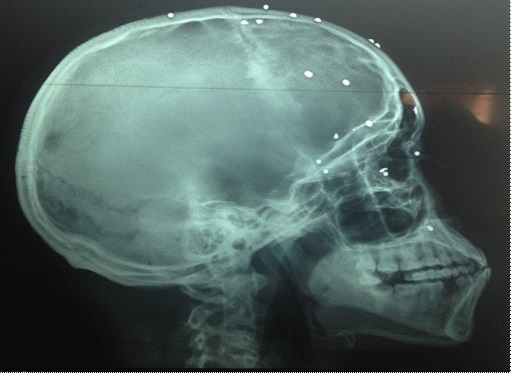
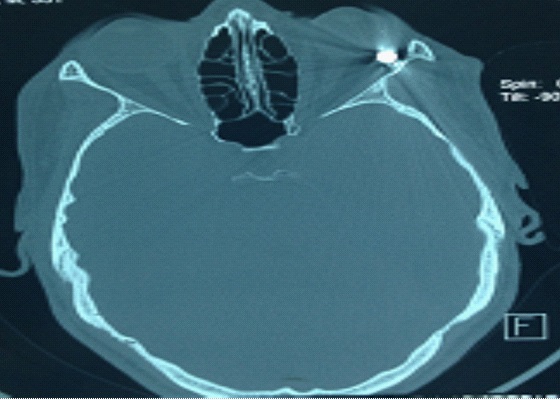
The B-Mode ocular ultrasound (10 MHz probe) confirmed vitreous hemorrhage and total Retinal Detachment (RD) in the Right Eye (RE) and partial retinal detachment in the Left Eye (LE) (Figure 1). X-ray of the nose bones and CT head showed several shot shots (Figure 2, Figure 3). The patient’s OTS was 2. He had been treated with anti-inflammatory drugs, antibiotics, extracapsular extraction and left eye vitrectomy. The evolution was stable.
Case 2
This was a 55-year-old patient, received for a painful red eye associated with a decrease in visual acuity, bilateral, following an assault by a shot gun, dating back to a week. The visual acuity was reduced to a LP+ in both eyes. He had diffuse subconjunctival hemorrhage, a 5-hour scleral wound, hypotonia, vitreous hemorrhage, and partial retinal detachment in both eyes. We had trimmed the scleral puncture wounds, after exploring the block, both eyes. CT head showed shot and B-scan ocular ultrasound, vitreous hemorrhage and retinal detachment. The patient’s OTS was 1. The evolution under surveillance was stable.
Case 3
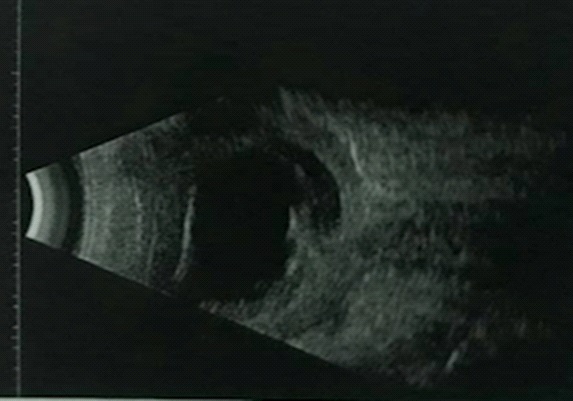
This was a 33-year-old patient, referred for a 03-month-old double-eyed decrease in visual acuity following a home-made gunshot trauma following an assault. The visual acuity was null with a lack of Light Perception (LP) on the right eye. The right eyeball was at the beginning of phthisis with athalamia, 360° irido-crystaline synechiae and hypotonia. Left visual acuity was reduced to LP+ with 5-hour adhesion leukemia and post-traumatic cataract.
B-scan ocular ultrasound confirmed phthysis of the right eye, vitreous hemorrhage with a total and old retinal detachment in both eyes (Figure 4). The progression under medical treatment was stable.
Case 4
A 35-year-old patient was received for a decreased visual acuity in left eye following a shotgun trauma following a robbery that took place two weeks ago. The visual acuity was reduced to LP. We understand a diffuse SCH (Figure 5), hypotonia and vitreous hemorrhage in left eye. The examination in the right eye was without particularity.

The orbits CT-scan showed an intraorbital shot and the OTS was 1. The evolution under medical treatment was stable.
Case 5
A 21-year-old patient was received because of a multiple ribbing of the right side of the face by shot during an assault, dating back to a week. On examination, visual acuity was reduced to LP- on the right eye. The patient had diffuse punctiform wounds of the right hemiface, diffuse SCH, stage 4 hyphema. Ocular tone was 10 mmHg. The left eye examination was normal. Bscan ocular ultrasound of the right eye showed an intraorbital shot likely responsible for the ocular lesions (Figure 5) and a deformation of the globe as well as a vitreo-retinal reshaping, probably corresponding to the exit door of the shot. CT head showed multiple cranio-facial granules (Figure 6). The OTS was 2. Hyphema resorption was obtained 4 days after medical treatment, with no improvement in visual acuity.

Table 1: Summary of individual cases of gunshot injuries.
Parameters |
Case 1 |
Case 2 |
Case 3 |
Case 4 |
Case 5 |
Age |
22 years |
55 years |
33 years |
35 years |
21 years |
Gender |
Male |
Male |
Male |
Male |
Male |
Reason for consultation |
Decreased visual acuity, ocular redness, eye pain at both eyes |
Decreased visual acuity, ocular redness, eye pain at both eyes |
Decreased visual acuity, ocular redness, eye pain at both eyes |
Decreased visual acuity, ocular redness, eye pain at left eye |
Decreased visual acuity, ocular redness, eye pain at right eye |
Consultation period |
1 week |
1 week |
3 months |
2 weeks |
1 week |
Visual acuity |
2 eyes= LP+ |
2 eyes= LP+ |
RE=LP+ |
LE=LP- |
RE=LP- |
Clinical examination |
SCH |
SCH |
RE: |
SCH, hypotonia, vitreous hemorrhage |
SCH, |
TDM |
Shots |
Shots |
Shots |
Shots |
Shots |
OTS |
2 |
1 |
|
1 |
2 |
Treatment |
Medico-surgical: antibiotics + antiinflammatory + extracapsular extraction + vitrectomy |
Medico-surgical: antibiotics + antiinflammatory |
Medical: antibiotics + antiinflammatory |
Medical: antibiotics + antiinflammatory |
Medical: antibiotics + antiinflammatory |
Prognosis |
poor |
poor |
poor |
poor |
poor |
Discussion
Gunshot eye injuries are the most common type of gunshot eye injury [1]. Several factors contribute to the spread of small arms and light weapons in Senegal. These factors can be exogenous and/or endogenous. These are the socio-political instability in the sub-region, the porosity of borders and the Senegalese socio-economic and cultural context (security, cultural rite, hunting activity). The carrying of arms in Senegal is governed by law 66-3 [5].
Firearm-related eye injuries in Senegal are infrequent. In our service, of 251 cases of ocular trauma, collected during the study period, 5 were related to shot weapons. LAM [6] had 4 weapons-related trauma cases out of 1,872 eye trauma cases.
In our series all subjects were male which is consistent with the classic predominance of trauma in the male subject.
These were young adults, the average age was 33.2 years with the extremes between 21 and 55 years. KOROBELNIK [7] in a 160-case study found an average age of 28 years. Reaching young people in full employment could have a socio-economic impact. Aggression was the main factor favouring [8].
The eye damage associated with shot guns is immediately severe. In our series, visual acuity was between LP- and LP+, consistent with the ASSAF and GAMBRELLE [1,8] studies that respectively had “counting fingers” VA and “see the hand movement” VA (VBM).
We had three bilateral forms and two unilateral forms. KOROBELNIK [7] found 110 unilateral and 50 bilateral cases. The distance of fire was not specified, however the cone shot with scattering of shot, this would explain the united or bilateral character of the ocular injuries.
According to the Birmingham Eye Trauma Terminology (BETT) [11], gunshot eye injuries are generally open-ended. In our series, all patients had open globe trauma, as well as in the ASSAF and GAMBRELLE studies [1,8]. This could be explained by the nature of the shot, which is rounded in shape and is projected by a secondary blast effect with a high kinetic velocity perforating the globe. KOROBELNIK [7] on a series of 160 cases or 310 eyes had observed 108 contused eyes.
OTS was less than or equal to 2 in four of our patients and our results are consistent with our prognosis. Indeed, with a score of 1, the probability of obtaining a visual acuity of 1/10 is 2% and 13% for a score of 2 [9].
No cases of endophthalmitis have been noted, which is comparable to the data in the literature since EHLERS [11] agrees that the blast-heated shot that propels them, constitute sterile foreign matter, exceptionally complicated of endophthalmos
Gunshot eye injuries are a poor prognosis. Thus, very low initial visual acuity remained stable in all of our patients. KOROBELNIK, as well as EHLERS [8,11] also point out that among the vulnerabilities traditionally responsible for perforating eye injuries, lead-based projectiles are particularly poor prognosis. Because of their spherical shape, the kinetic energy of lead must be very high for it to perforate the eye, so the eye damage caused is often major. However, BERTIN [12] notes an improvement in visual acuity and this difference is certainly due to the early management, which was not the case for our patients who came late for consultation.
Conclusion
Gunshot eye injuries are on the rise. Facial screening is all the severity of these traumas involving functional prognosis and young people in full professional activity are mainly concerned. The reduction in the use of these weapons will be achieved by strengthening the legislative provisions governing the possession of firearms.
References
- Assaf E. Armes à grenailles, une menace oculaire qui persiste. Jr Fr Opht. 2003; 26: 960-966.
- Hadden WA, Rutherford W, Merret JD. The injuries of terrorist bombing: A patient. Br J Surg. 1978; 65: 525-531.
- Mallonee, Shariat S. Physical injuries and facilities resulting from the Oklahoma City bomning. JAMA. 1996; 276: 382-387.
- Kuhn F, Maisiak R, Mann L, Mester V, Morris R, Witherspoon CD, et al. The Ocular Trauma Score (OTS). Ophthalmol clin north Am. 2002; 15: 163-165.
- Bathily DA. Problématique de la dissémination des armes légères et de petit calibre au Sénégal MALAO Sénégal, Décembre 2012.
- Lam A. Traumatismes oculaires au Sénégal, bilan épidémiologique et statistique de 1872 cas. Med Afrique Noire. 1992; 39: 810-815.
- Korobelnik JF, Cetinel B, Frau E, chauvaud D, Pouliquen Y. Lésions oculaires par pistolet à grenailles. Etude épidémiologique de 160 patients. J fr Ophtalmol avril 1993; 16: 453-7.
- J Gambrelle, V Sebilleau, Fleury J, Denis P. Chirurgie des traumatismes oculaires perforants du segment postérieur par plomb: A propos de 2 cas. J fr Ophthalmol. 2010; 33: 397-402.
- Kuhn F, Morris R, Witherspoon CD. Birmingham Eye Trauma Terminology. Ophthalmol clin North Am. 2002; 15: 139-142.
- Boscher–southall CI, Manderieux N, Konqui P, Pouliquen Y, et al. Traumatismes oculaires par grenailles de plomb et plombs de chasse. A propos de 38 cas. Bull Soc Opht France. 1988; LXXXVIII: 195-200.
- Ehlers JP, kunimoto DY, Ittoop S, Maguire Jl , Ho AC, Regillo CD. Metallic intraocular foeign bodies: Chararteristics, interventions, and pronostic factors for visual outcoe and globe survival. Am J Ophthalmol. 2008; 146: 427-433.
- Bertin V, Barale PO, Hamard H. Criblages oculaires perforants et pistolets à grenailles. Ophtalmologie. 1995; 9: 378-380.