
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Post-intubation tracheoesophageal fistula in severe SARS-CoV-2 - COVID-19 patient: Unexpected finding during swallowing test
Fabrizia Elli
Division of Otorhinolaryngology, Department of Biotechnology and Life Sciences, University of Insubria, Ospedale di Circolo e Fondazione Macchi, Via Guicciardini 9, 21100, Varese, Italy
*Corresponding Author: Fabrizia Elli
Division of Otorhinolaryngology, Department of Biotechnology and Life Sciences, University of Insubria,
Ospedale di Circolo e Fondazione Macchi, Via Guicciardini 9, 21100, Varese, Italy
Email: fabrizia.elli@hotmail.it
Received : Mar 28, 2022
Accepted : Apr 22, 2022
Published : Apr 29, 2022
Archived : www.jcimcr.org
Copyright : © Elli F (2022).
Abstract
Introduction: COVID-19 pandemic, caused by severe acute respiratory syndrome coronavirus 2, led to an increase in intensive care admission for massive interstitial pneumonia. Many patients underwent long periods of endotracheal intubation for mechanical ventilation and subsequent tracheostomy. The most common complications related to these maneuvers are known: laryngotracheal granulomas, webs, stenosis and malacia. Less common complications are tracheal necrosis with trachea-esophageal or tracheo-arterial fistulas, caused by compression between the orotracheal tube cuff and the nasogastric tube.
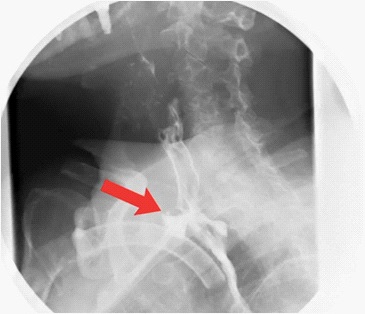
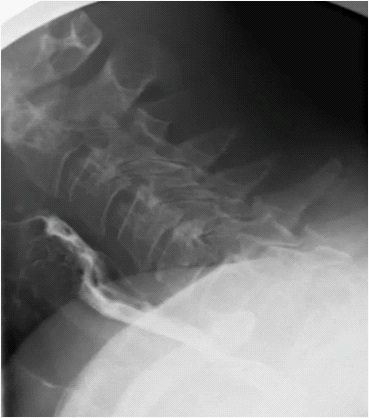
Case report: We present the case of a patient with severe COVID-19 associated pneumonia who underwent orotracheal intubation and prolonged mechanical ventilation for two months with unexplained episodes of food inhalation. During the swallowing test, it was observed inhalation, without natural passage of food from the glottic plane. Therefore, ENT specialist in swallowing, suspecting the feared tracheo-esophageal fistula, requested a double contrast esophageal xray that confirmed the diagnostic hypothesis. Thoracic surgery team performed surgical correction by resection and tracheal anastomosis with esophagoraffia.
Discussion: TEF is a very rare, but potentially fatal, complication of invasive VM. Predisposing factors are prolonged periods of invasive VM, elevated cuff pressures, oversized endotracheal tubes, patient comorbidities, local and general infections, use of a nasogastric tube. The endoscopic swallow test is a relatively simple test, performed at the patient’s bed, that can identify oropharyngeal swallowing disorders and esophageal changes, such as tracheoesophageal fistula.
Citation: Elli F. Post-intubation tracheoesophageal fistula in severe SARS-CoV-2 - COVID-19 patient: Unexpected finding during swallowing test. J Clin Images Med Case Rep. 2022; 3(4): 1813.
Introduction
The SARS-CoV-2 pandemic has spread dramatically and rapidly around the world. This disease is a highly contagious pandemic zoonosis caused by an RNA beta-coronavirus. In most patients, the disease takes a mild form with symptoms such as fever, cough, nausea, vomiting, and diarrhea. However, in some individuals, it can cause massive involvement of the lower respiratory tract resulting in interstitial pneumonia [1]. Despite the low mortality rate (1.4-2.3%) [2] and the relatively low number of patients requiring intensive care (between 5 and 12%), due to its high transmissibility the infection has challenged the global healthcare system [3]. There has been unprecedented overcrowding of hospital facilities, particularly intensive care units (ICUs). This followed the development of severe hypoxemia related to acute respiratory distress syndrome (60-70% of cases), shock (30%), myocardial dysfunction (20-30%), and acute renal failure (10-30%) [4].
The significant increase in the number of patients requiring admission to intensive care units (ICUs) and prolonged invasive mechanical ventilation (MV) has brought to light an important number of complications. The most common are: laryngotracheal granulomas, spider webs, stenosis, malacia up to tracheal necrosis with trachea-esophageal or tracheo-arterial fistulas [5].
Case report
We report the case of a COVID-19 patient who underwent prolonged invasive VM for two months and developed FET. Tracheoesophageal fistula (TEF) is a connection between the trachea and esophagus, which can be congenital or acquired. TEF following prolonged invasive VM is a rare condition, with an incidence of 0.3-3% [6].
A 58-year-old female patient with a prior history of hypertension and ovarian carcinoid presented to the emergency department (ED) in May 2021, complaining of dyspnea and cough for several days. On admission, she tested positive for severe acute respiratory syndrome coronavirus 2 (SARS CoV-2). Clinical, laboratory and imaging examinations confirmed the diagnosis of pneumonia associated with SARS CoV-2, with severe hypoxemic respiratory failure.
The patient was therefore admitted to the intensive care unit and was intubated and mechanically ventilated. However, the clinical evolution was unfavorable with persistent PaO2 /FiO2 ratio <150 and the patient underwent percutaneous tracheostomy and PEG placement. In September 2021, during rehabilitation, performed by speech therapist specializing in swallowing disorders, uncommon swallowing alterations appeared. Therefore, the patient underwent specialized ENT evaluation by endoscopic endonasal swallowing test with food of various densities. During the examination, normal oro-pharyngeal transit was initially observed, with subsequent onset of coughing and tracheal bolus ascension. The fibroendoscope was therefore removed to allow the patient to adequately clear the ingestions. At the subsequent re-evaluation, no traces of food residues were found in the laryngeal vestibule. This finding led to the suspicion of the presence of a passage between the esophagus and trachea. So, the specialist recommended a double-contrast esophageal Xray with video-recorded swallowing study confirming a tracheoesophageal fistula of the cervical esophageal portion. The thoracic surgery team, after identifying and evaluating the FET by bronchoscopy and gastroscopy, performed surgical correction by resection and tracheal anastomosis with esophagorrhaphy, re-establishing the correct anatomical boundaries.

Discussion
Acquired TEF is a rare but potentially serious complication of prolonged intubation for mechanical ventilation. Several factors facilitate its development: high cuff pressures, oversized endotracheal tubes, patient comorbidities, corticosteroid use, local infections, nasogastric tube, need to change position (prone supine) frequently with possible excessive tube movement, repeated bronchoscopies, high PEEP ventilation over a period of 4 weeks [7,8].
The classic presentation of TEF is represented by a sudden drop in oxygen saturation, despite adequate ventilation, associated with positive cuff leakage and gastric distension.
This was not the case in our case, but the presence of fistula was suspected only during fiberoptic endoscopic evaluation of swallowing (FEES). During the examination, there was an episode of massive inhalation with food at tracheal, level without observing bolus at subglottic glottic level in absence of frank regurgitation or alteration of the epiglottic tilt.
Despite the high morbidity and mortality of TEF, which is even higher in patients with COVID-19, surgical repair is generally required because spontaneous closure of a FET is rare [9].
Conclusion
In summary, a COVID-19 patient with respiratory failure developed a FET that was only suspected during swallow testing, as he had not previously given symptoms. This suggests that, alongside radiological (CT) or operative (bronchoscopy) examinations [10], a relatively simple and inexpensive examination such as endoscopic swallowing testing may have diagnostic value. The advantages of this test are the possibility to perform it at the patient’s bedside, the low complications, and the reproducibility over time. So, in this way, it is possible to identify oropharyngeal swallowing disorders and esophageal alterations, such as tracheoesophageal fistula, and monitor their evolution or regression over time.
References
- Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of Coronavirus disease 2019 in China. N Engl J Med 2020; 382: 1708-1720.
- Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel Coronavirus-infected pneumonia in Wuhan. JAMA. 2020; 323: 1061-1069.
- Kowalski LP, Sanabria A, Ridge JA, et al. COVID-19 pan- demic: Effects and evidence-based recommendations for otolaryngology and head and neck surgery practice. Head Neck. 2020. https:// doi.org/10.1002/hed.26164
- Phua J, Weng L, Ling L et al (2020) Intensive care management of Coronavirus disease 2019 (COVID-19): challenges and recommendations. Lancet Respir Med. 2020; 8: 506-517.
- Nikolovski N, Kopacheva-Barsova G, Pejkovska A. Laryngotracheal stenosis: a retrospective analysis of their aetiology, diagnose and treatment. Open Access Maced J Med Sci. 2019; 7: 1649- 1656.
- Couraud L, Ballester MJ, Delaisement C. Acquired tracheoesophageal fistula and its management. Semin Thorac Cardiovasc Surg. 1996; 8: 392-9.
- M Wolf, E Segal, A Yellin, M Faibel, YP Talmi, J Kronenberg. Acquired tracheoesophageal fistula in critically ill patients,” The Annals of Otology, Rhinology, and Laryngology. 2016; 109(8): 731-735.
- Mehel DM, Ozdemir D, Çelebi M, Aydemir S, Akgul G, Ozgur A. Classification of laryngeal injury in patients with prolonged intubation and to determine the factors that cause the injury. Am J Otolaryngol. 2020; 41: 102432.
- G Marulli, M Loizzi, G Cardillo, L Battistella, A De Palma, P Ialongo, et al. Early and late outcome after surgical treatment of acquired non-malignant tracheo-oesophageal fistulae, European Journal of Cardio-Thoracic Surgery. 2013; 43(6): e155–e161. https://doi.org/10.1093/ejcts/ezt069.
- RC Mooty, P Rath, M Self, E Dunn, A Mangram. Review of tracheo-esophageal fistula associated with endotracheal intubation. Journal of Surgical Education. 2007; 64(4): 237-240.