
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Classical bladder exstrophy in an adult female
Adil Mellouki1,2*; Ouima Justin Dieudonné ZIBA1,2; Mustapha Ahsaini1,2; Soufiane Mellas1,2; Jalal Eddine El Ammari1,2; Mohammed Fadl Tazi1,2; Mohammed Jamal El Fassi1,2; Moulay Hasan Farih1,2
1 Department of Urology, Hassan II University Hospital, Fez, Morocco.
2 Faculty of Medicine, Pharmacy and Dentistry of Fez, Sidi Mohammed Ben Abdellah University, Morocco.
*Corresponding Author: Adil Mellouki
Urology Department, CHU of Fez, Sidi Mohammed
Ben Abdellah University, Fez, Morocco.
Email: Adil.mellouki@gmail.com
Received : Mar 31, 2022
Accepted : Apr 26, 2022
Published : May 03, 2022
Archived : www.jcimcr.org
Copyright : © Mellouki A (2022).
Citation: Adil M, Ouima JDZ, Mustapha A, Soufiane M, Jalal EEA, et al. Classical bladder exstrophy in an adult female. J Clin Images Med Case Rep. 2022; 3(5): 1816.
Clinical image description
Classical bladder exstrophy results from a defective lower abdominal wall with open bladder and urethra, and anteriorly opened bony pelvis [1]. Families with low socioeconomic status, lack of education and limited access to health care in developing countries often neglect treatment of such cases [2].
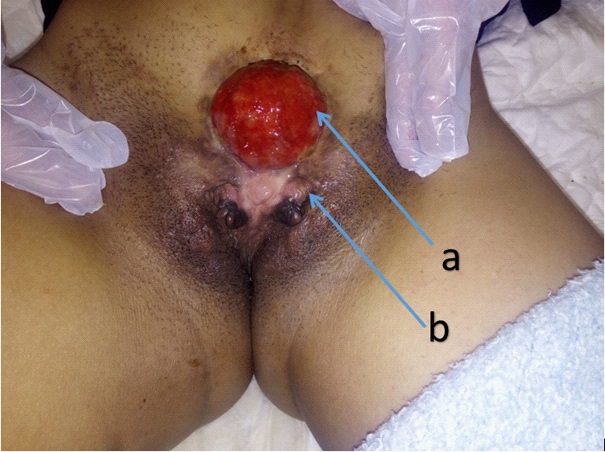
We present the case of a 28-year-old female patient, single, with low socioeconomic status, no notion of consanguinity, and no similar cases in the family. She had a bladder exstrophy since birth, never treated. She consulted for urinary incontinence. On clinical examination (Figure 1): presence of a 4.5 cm bladder template with fibrotic inflammatory mucosa between the two rectus muscles; ureter ostia noticeable with nipples. No umbilicus, no vaginal orifice. On radiographic exploration of the pelvis: enlargement of the iliac bones, a vaginal imperforation was objectified on MRI, the biopsy of the plaque was in favor of normal skin tissue, with a discrete lesion of non-specific chronic cystitis. Therapeutically, the patient refused the surgical procedure and was discharged against medical advice.
Conflict of interest: The authors declare that they have no conflicts of interest in relation to this paper.
References
- Inouye BM, Massanyi EZ, Di Carlo H et al. Modern Management of Bladder Exstrophy Repair. Curr Urol Rep. août. 2013; 14(4): 359-65.
- Kiran PS, Panaiyadiyan S, Singh P et al. Management of Untreated Classical Bladder Exstrophy in Adults: A Single-Institutional Experience. Urology. 2020; 146: 293‑8.