
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A solitary gastric metastasis originating from primary nasal mucosal melanoma treated with wedge gastrectomy
Ioannis Spyrou1; Eftychia Chatziioannou2; Tania Triantafyllou1*; Georgios Zografos1; Dimitrios Theodorou1
1 Department of Surgery, Hippocration General Hospital of Athens, National and Kapodistrian University of Athens, Athens, Greece.
2 Medical School of Athens, National and Kapodistrian University of Athens, Athens, Greece.
*Corresponding Author: Tania Triantafyllou
Department of Surgery, Hippocration General Hospital of Athens, National and Kapodistrian University of Athens, Athens, Greece.
Email: t_triantafilou@yahoo.com
Received : Apr 01, 2022
Accepted : Apr 27, 2022
Published : May 04, 2022
Archived : www.jcimcr.org
Copyright : © Tania Triantafyllou (2022).
Abstract
Sinonasal melanoma is a rare type of melanoma that originates from the mucous membranes of the nasal and paranasal sinuses. It has a poor prognosis with an estimated 5-year overall survival rate of 10- 30%. The most common locations of metastasis include lymph nodes, liver and lungs. Currently, there are several therapeutic options for advanced mucosal melanoma. We report a case of a 77-year-old male patient who presented to our surgical department with acute vague postprandial abdominal pain one year after excision of a sinonasal mucosal melanoma (MM). Upper gastrointestinal (GI) endoscopy revealed a 2 cm solitary ulcerated polypoid lesion. Histological examination and immunohistochemistry confirmed the diagnosis of metastatic melanoma. Wedge gastrectomy was performed, and the tumor was excised with histologically confirmed negative margins. To our knowledge, this is the first case of gastric metastasis from primary nasal melanoma, the most common type of head and neck mucosal melanoma, described in the literature. The stomach is a rare metastatic site for both cutaneous and mucosal melanomas. Non-specific gastrointestinal symptoms in a patient with a history of nasal melanoma should be investigated, as excision and systemic therapy including immunotherapy and targeted therapy may improve patient survival.
Keywords: Nasal melanoma; Solitary gastric metastasis; Wedge gastrectomy; Checkpoint inhibitor immunotherapy; Targeted therapy.
Abbreviations: 18F-FDG: fluorodeoxyglucose F 18; AJCC: American Joint Committee on Cancer; CDK: Cyclin-dependent kinase; CTLA-4: cytotoxic T-lymphocyte-associated protein 4; GI: gastrointestinal; MM: mucosal melanoma; PD-1: Programmed cell death protein 1.
Citation: Ioannis S, Eftychia C, Tania T, Georgios Z, Dimitrios T. A solitary gastric metastasis originating from primary nasal mucosal melanoma treated with wedge gastrectomy. J Clin Images Med Case Rep. 2022; 3(5): 1818.
Introduction
Mucosal melanoma accounts for 1% of melanomas. Apart from ocular, it includes head and neck melanomas (50%), gastrointestinal, anorectal, genitourinary and respiratory melanomas [1,2]. Head and neck mucosal melanoma is found in paranasal and nasal cavities, mouth, larynx, pharynx and upper esophagus. The nasal and paranasal sinuses are the most frequent localizations [3]. Nasal melanoma occurs with decreasing frequency in the lateral nasal wall, inferior turbinate and anterior nasal septum, while the paranasal sinuses are less frequently affected and mainly involve the maxillary and ethmoid sinuses. Mucosal melanoma has a less favorable prognosis compared to cutaneous melanoma. The tumor can be pigmented or, less frequently, amelanotic. The presenting symptoms are non-specific and include epistaxis and nasal obstruction symptoms. Local recurrence after initial excision is common and is associated with a higher risk of distant metastasis. The liver, lungs and lymph nodes are the most common metastatic sites [3].
Case presentation
A 77-year-old male patient presented to our surgical department with acute vague postprandial abdominal pain, one year after excision of a sinonasal mucosal melanoma. The medical history included chronic obstructive pulmonary disease and ulcerative colitis, which was medically managed and under remission. The patient was a smoker with 120 pack-years.
The primary tumor was located between the superior and middle turbinate in the lateral wall of the right nasal cavity. The tumor was excised with histologically confirmed negative margins. The pathology report showed squamous epithelium invaded by malignant cells, magenta-colored nuclei of different sizes, prominent nucleoli, nuclear atypia, increased mitotic rate (>10 mitoses/mm2 ) and atypical mitoses. Immunohistochemistry demonstrated cell positivity for MelanA, HMB-45, vimentin, S-100 and MITF. The Ki67 index was >60%. Adjacent structures were not infiltrated and no locoregional or distant metastases were found. According to the seventh edition of the American Joint Committee on Cancer (AJCC) for head and neck mucosal melanoma, the diagnosis was stage III primary nasal melanoma (T3, N0, M0) and no further excision or radiotherapy was required. The patient was referred to the oncology unit for further consultation and treatment.
Local recurrence was diagnosed in the third and ninth months after the first resection (stage IVA (T4a, N0, M0). They were endoscopically resected with negative margins and antiCTLΑ-4 immunotherapy was administered. No further residual or recurrent disease was detected at follow-up visits.
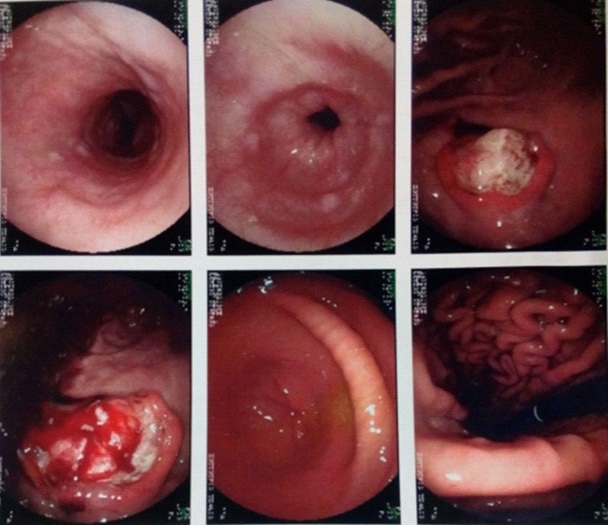
The patient presented to our surgical department 4 months after the second local recurrence. Physical examination revealed vague abdominal pain. We performed an upper gastrointestinal (GI) tract endoscopy (Figures 1,2). A solitary 2 cm polypoid, ulcerated lesion along the greater curvature of the stomach was revealed. Immunohistochemistry of the bioptic specimen was positive for S-100 and MelanA. In addition, the patient underwent a PET-CT scan, which showed increased fluorodeoxyglucose F 18 (18F-FDG) uptake at the border between the corpus and the fundus along the greater curvature of the stomach. A detailed dermatologic examination and the PET-CT scan excluded other metastases.
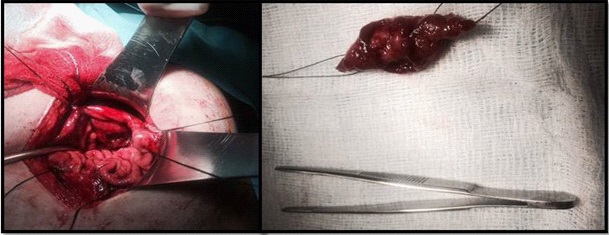
A wedge gastrectomy was performed, and the tumor was removed with histologically confirmed negative margins. The pathology report of the surgical specimen was conclusive of melanoma metastasis. Immunohistochemistry revealed heterogeneous positivity for MelanA and HMB-45. The patient was discharged on the sixth postoperative day and remains diseasefree three months after surgery.
Discussion
Sinonasal melanoma is a rare entity accounting for 1% of melanomas. It originates from melanocytes lining the mucous membranes of the nasal and sinonasal sinuses. Mucosal melanoma differs from cutaneous melanoma in that it has a distinct molecular profile and a poorer prognosis. It is more common in females in their seventh decade of life. It can be either pigmented or amelanotic [4]. Its poor prognosis is reflected in the current classification system, as all head and neck mucosal melanomas are classified as either stage III or IV, whereas stages I and II do not exist. A stage III tumor is confined to the mucosa and the underlying soft tissue (T3, N0, M0). Stage IV refers to advanced tumors (T4a and T4b) or when lymph node or distant metastases are present. Gal et al. reported a 5-year survival rate of 40% for stage III and between 10 and 20% for stage IV. Locoregional or distant relapse develops in 80% of cases after initial resection [5].
The optimal treatment for primary sinonasal melanoma is wide excision with microscopically confirmed negative margins and if R0 excision is not possible, radiotherapy is offered. Sentinel lymph node biopsy is not routinely performed, and lymph node dissection is performed if lymph nodes are clinically involved. Treatment of stage IV consists mainly of systemic therapy. Due to the rarity of cases, there have been no large studies assessing stage IV mucosal melanoma treated with metastasectomy. It has been showed that metastasectomy improves survival in cutaneous melanoma [6]. Bello et al. showed a better prognosis for melanoma patients, including mucosal melanoma patients, who underwent metastasectomy after administration of immunotherapy [7]. Systemic therapy consists of immunotherapy, targeted therapy and participation in clinical trials. Immunotherapy with PD-1 and CTLA-4 checkpoint inhibitors provides a survival benefit for mucosal melanoma patients. In the CheckMate-067 trial, the 5-year response rate for ipilimumab (CTLA-4 inhibitor) and nivolumab (PD-1 inhibitor) was 43% compared to 30% for nivolumab and 7% for ipilimumab alone [8]. Targeted therapies with BRAF and MEK inhibitors are another option, although BRAF and NRAS mutations are not as common as in cutaneous melanoma [9]. Moreover, c-KIT inhibitors are an alternative, as 30-40% of mucosal melanomas have c-KIT activating mutations and amplifications [10]. In addition, copy number alterations in the Cyclin- dependent kinase 4 (CDK4) pathway are found in mucosal melanoma and the use of CDK4/6 inhibitors is being investigated in this type of melanoma [11]. Clinical trials combining immune checkpoint inhibitors and other targeted therapies exist. Thus, prompt detection of metastatic disease is important, and sequencing of metastatic lesions may indicate whether targeted therapy should be considered.
According to the existing literature, gastric metastases are rare in cutaneous and ocular melanomas [12-14]. Cases of mucosal melanomas developing gastric metastasis are limited. Cases of vulvovaginal, oral and sphenoid sinus melanomas developing gastric metastasis have been reported [15-19]. Gastric metastases are challenging to diagnose because of their nonspecific symptoms. They are more often multiple, ulcerated, located in the submucosa and develop in a widespread metastatic setting [20,21]. They are pigmented or amelanotic, the latter being more difficult to diagnose. Nevertheless, as far as we know, gastric metastasis has not been reported in primary nasal melanoma. In the present case, the stomach was the first distant metastatic lesion and presented as a solitary, amelanotic tumor. The diagnosis was made based on the medical history and the directed immunohistochemistry.
Conclusion
In conclusion, we present a rare case of primary nasal melanoma resulting in a solitary distant gastric metastasis treated with wedge gastrectomy. To our knowledge, this is the only case reported in the literature that originated from a primary nasal melanoma and was considered important as nasal melanoma is the most common type of head and neck mucosal melanoma. With this case report, we would like to highlight that clinicians should maintain a high level of suspicion for non-specific gastrointestinal symptoms in patients with a medical history of mucosal or cutaneous melanoma. Timely diagnosis is key to treatment, as several therapeutic alternatives are available.
Conflicts of interest: The authors declare that they have no conflict of interest to disclose.
References
- Spencer KR and Mehnert JM. Mucosal Melanoma: Epidemiology, Biology and Treatment. Cancer Treat Res. 2016; 167: 295- 320.
- Dominiak NR, Wick MR and Smith MT. Mucosal melanomas: Site-specific information, comparisons with cutaneous tumors, and differential diagnosis. Semin Diagn Pathol. 2016; 33(4): 191- 197.
- Lian B, Cui CL, Zhou L, Song X, Zhang XS, Wu D, et al. The natural history and patterns of metastases from mucosal melanoma: an analysis of 706 prospectively-followed patients. Ann Oncol. 2017; 28 (4): 868-873.
- Pontes FSC, de Souza LL, de Abreu MC, Fernandes LA, Rodrigues ALM, do Nascimento DM, et al. Sinonasal melanoma: a systematic review of the prognostic factors. Int J Oral Maxillofac Surg. 2020; 49 (5): 549-557.
- Gal TJ, Silver N and Huang B. Demographics and treatment trends in sinonasal mucosal melanoma. Laryngoscope. 2011; 121 (9): 2026-2033.
- Majem M, Manzano JL, Marquez-Rodas I, Mujika K, MuñozCouselo E, Pérez-Ruiz E, et al. SEOM clinical guideline for the management of cutaneous melanoma (2020). Clin Transl Oncol. 2021; 23 (5): 948-960.
- Bello DM, Panageas KS, Hollmann T, Shoushtari AN, Momtaz P, Chapman PB, et al. Survival Outcomes After Metastasectomy in Melanoma Patients Categorized by Response to Checkpoint Blockade. Ann Surg Oncol. 2020; 27 (4): 1180-1188.
- Shoushtari A, Wagstaff J, Ascierto P, Butler M, Lao C, MarquezRodas I, et al. CheckMate 067: Long-term outcomes in patients with mucosal melanoma. 2020.
- Gutiérrez-Castañeda LD, Nova JA and Tovar-Parra JD. Frequency of mutations in BRAF, NRAS, and KIT in different populations and histological subtypes of melanoma: a systemic review. Melanoma Res. 2020; 30 (1): 62-70.
- Kim KB and Alrwas A. Treatment of KIT-mutated metastatic mucosal melanoma. Chin Clin Oncol 2014; 3 (3): 35.
- Xu L, Cheng Z, Cui C, Wu X, Yu H, Guo J, et al. Frequent genetic aberrations in the cell cycle related genes in mucosal melanoma indicate the potential for targeted therapy. J Transl Med. 2019; 17 (1): 245.
- Cohen VM, Ahmadi-lari S and Hungerford JL. Gastric metastases from conjunctival melanoma. Melanoma Res. 2007; 17 (4): 255- 256.
- Ueno N, Yoneda M, Inamori M and Imai N. Metastatic malignant melanoma in the upper alimentary tract. Gastrointestinal Endoscopy. 2006; 64 (6): 1002-1003.
- Liang KV, Sanderson SO, Nowakowski GS and Arora AS. Metastatic malignant melanoma of the gastrointestinal tract. Mayo Clin Proc. 2006; 81 (4): 511-516.
- Matsubayashi H, Takizawa K, Nishide N and Ono H. Metastatic Malignant Melanoma of the Gastric Mucosa. Internal Medicine. 2010; 49 (12): 1243-1244.
- Inamori M, Ueno N, Fujita K, Fujisawa T, Fujisawa N, Yoneda M, et al. Gastrointestinal: Gastrointestinal metastases from malignant melanoma. Journal of Gastroenterology and Hepatology. 2006; 21 (1): 327-327.
- Mostafa MG, Hussein MR, El-Ghorory RM and Gadullah HA. Gastric metastases from invasive primary mucosal epithelioid malignant melanoma of the hard palate: report of the first case in the English literature. Expert Rev Gastroenterol Hepatol. 2014; 8 (1): 15-19.
- Ton L, Sidhu G, Almouradi T, Mishra S and Attar B. A Rare Case of Oral Malignant Melanoma with Gastrointestinal Metastases: 1559. American Journal of Gastroenterology. 2016; 111: S722- S723.
- Zhao L, Yan J, Li L, Wei J, Li L, Qian X, et al. Gastric metastasis from sphenoid sinus melanoma: A case report. Oncol Lett. 2015; 9 (2): 609-613.
- Langner C. [Secondary tumors of the gastrointestinal tract]. Pathologe. 2012; 33 (1): 45-52.
- McDermott VG, Low VH, Keogan MT, Lawrence JA and Paulson EK. Malignant melanoma metastatic to the gastrointestinal tract. AJR Am J Roentgenol.1996; 166 (4): 809-813.