
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Flashes and floaters as only sign of underlying retinal tear and vitreous hemorrhage
Wei Chen Lai1; Timothy Lee2*; Sidney A Schechet1,3
1 University of Maryland School of Medicine, Baltimore, MD, USA.
2 Uniformed Services, University of the Health Sciences School of Medicine, Bethesda, MD, USA.
3 Elman Retina Group, Baltimore, MD, USA.
*Corresponding Author: Timothy Lee
Uniformed Services University of the Health Sciences School of Medicine, Bethesda, MD, USA.
Email: tlee18504@gmail.com
Received : Mar 31, 2022
Accepted : Apr 28, 2022
Published : May 05, 2022
Archived : www.jcimcr.org
Copyright : © Lee T (2022).
Citation: Wei CL, Timothy L, Schechet SA. Flashes and floaters as only sign of underlying retinal tear and vitreous hemorrhage. J Clin Images Med Case Rep. 2022; 3(5): 1820.
Description
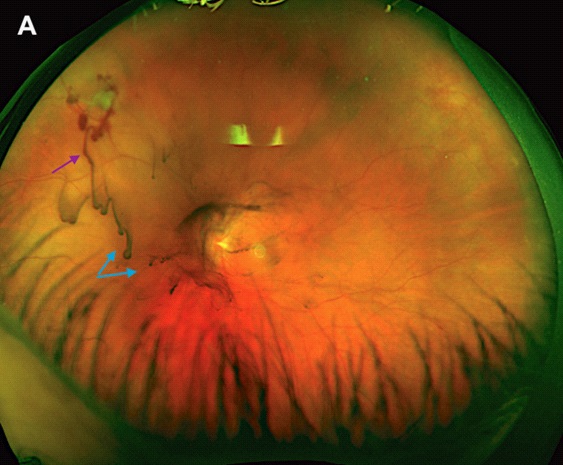
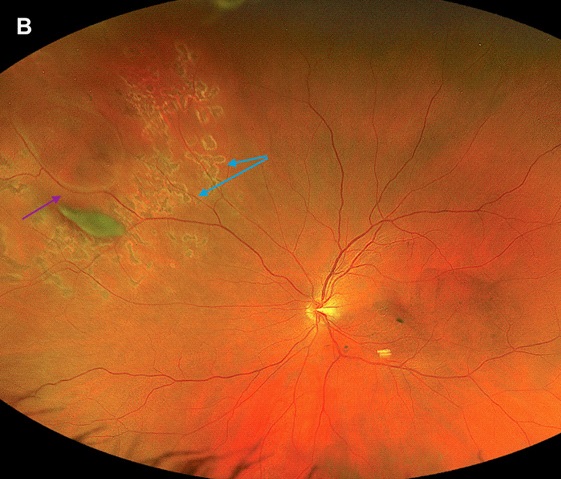
A 54-year-old myopic female presented with sudden flashes/ floaters in her left eye. Visual acuity was 20/20 and 20/80 in the right and left eye, respectively. Dilated exam of the left eye revealed posterior vitreous detachment (PVD), a retinal tear at 10 o’clock with an actively-bleeding bridging vessel (Figure 1, purple arrow), and a mild vitreous hemorrhage (VH) (Figure A, blue arrows). She was diagnosed with hemorrhagic PVD secondary to an acute retinal tear in the left eye. Laser retinopexy was performed immediately to prevent retinal detachment (RD). On follow-up, the retina remained flat with good laser scarring barricading the tear, successfully preventing RD (Figure 1).
Key symptoms of a PVD are acute onset of flashes and floaters. PVD is a physiologic change due to aging where the vitreous degenerates, liquifies, and separates from the retina [1]. If the vitreous adheres strongly to and aggressively pulls the retina, dramatic increases in flashes and floaters are often first signs of structural retinal damage such as a retinal tear [2].
PVD’s naturally occur but portend a 5-10% of associated retinal tears, leading to RD if untreated [3]. In about 7.5% of PVDs, a retinal blood vessel can be torn, causing hemorrhage. A hemorrhagic PVD increases risk of having an underlying retinal tear to nearly 70% and further worsens visual acuity [3,4]. Retinal tears can lead to blinding retinal detachments, so diagnosing and treating a tear promptly is paramount to preserving vision. When a PVD occurs without retinal tear or detachment, close monitoring is recommended, for tears can occur within a few months of PVD occurrence.
Given the serious conditions that could cause flashes/floaters, first-line management in patients presenting with acute flashes/floaters is an urgent ophthalmologic assessment. A complete dilated eye exam within 24 hrs of symptom onset is recommended for ophthalmologists to evaluate, diagnose, and prevent potentially serious blinding conditions.
References
- Gishti O, Van den Nieuwenhof R, Verhoekx J, van Overdam K. Symptoms related to posterior vitreous detachment and the risk of developing retinal tears: a systematic review. Acta Ophthalmol. 2019; 97(4): 347-352. doi:10.1111/aos.14012.
- Sharma P, Sridhar J, Mehta S. Flashes and Floaters. Prim Care. 2015; 42(3): 425-435. doi:10.1016/j.pop.2015.05.011.
- Bond-Taylor, Martin et al. Posterior vitreous detachment - prevalence of and risk factors for retinal tears. Clinical ophthalmology (Auckland, NZ). 2017; 11: 1689-1695. doi:10.2147/OPTH. S143898.
- Sarrafizadeh R, Hassan TS, Ruby AJ, et al. Incidence of retinal detachment and visual outcome in eyes presenting with posterior vitreous separation and dense fundus-obscuring vitreous hemorrhage. Ophthalmology. 2001; 108(12): 2273-2278. doi:10.1016/s0161-6420(01)00822-3.