
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Unilateral bullous emphysema after successful treatment of a malignant pleural mesothelioma with combined CTLA-4 and PD-1 blockade
Toy HI1*; Misch D1,4; Stephan-Falkenau S3; Althoff CE4; Gebhardt A1,4; Bauer TT1,4; Kollmeier J1,4
1 Respiratory Diseases Clinic Heckeshorn, Helios Clinic Emil von Behring, Berlin, Germany
2 Berlin Lung Institute, Berlin, Germany.
3 Department of Tissue Diagnostics, Helios Klinikum Emil von Behring, Berlin, Germany.
4 Department of Radiology and Nuclear Medicine, Berlin, Germany
*Corresponding Author: Halil Ibrahim Toy
Respiratory Diseases Clinic Heckeshorn, Helios Clinic
Emil von Behring, Berlin, Germany.
Email: toyibrahim@posteo.de
Received : Mar 31, 2022
Accepted : Apr 28, 2022
Published : May 05, 2022
Archived : www.jcimcr.org
Copyright : © Toy HI (2022).
Citation: Toy HI, Misch D, Stephan-Falkenau S, Althoff CE, Gebhardt A, et al. Unilateral bullous emphysema after successful treatment of a malignant pleural mesothelioma with combined CTLA-4 and PD-1 blockade. J Clin Images Med Case Rep. 2022; 3(5): 1821.
Clinical Image
The malignant pleural mesothelioma (MPM) originates from the mesothelial tissue of the pleura and is associated with exposure to asbestos in majority of cases. Genetic susceptibility and potential synergy with an infection with the Simian Virus 40 are discussed for the pathogenesis of MPM [1].
Patients present with the onset of nonspecific symptoms such as dyspnea on exertion, due to pleural effusions, shortness of breath, chest wall pains and cough [2]. Diagnostic procedures such as CT-scans, followed up by a CT guided core biopsy or video-assisted thoracoscopic (VATs) guided pleural biopsy are recommended. Specific biomarkers are not validated yet for the diagnosis and prognosis. Current treatment options include chemotherapy, surgical treatment and radiotherapy and stable disease is the usual response [3]. The combined checkpoint inhibitor therapy has been introduced into clinical routine during 2021 [4] .
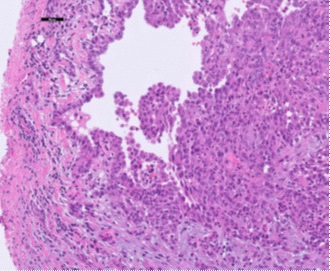
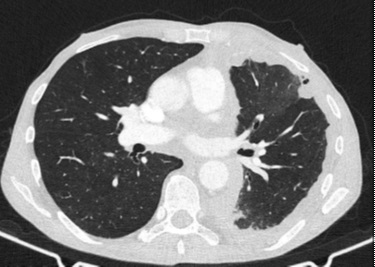
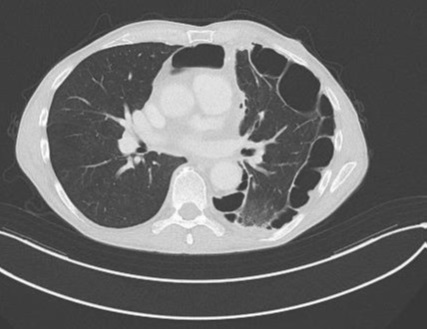
We present a 65 year old patient who was diagnosed with epithelioid MPM in February 2021 (Figure 1). A positron emission tomography with F-FDG as a radiotracer showed a metabolically active mass at the level of the left lower lobe and the dorsobasal recess with infiltration of the dorsal thoracic wall. We confirmed diagnosis via VATs guided pleural biopsy and achieved pleurodesis. The tumor board recommended a multidisciplinary approach with initiation of chemotherapy (ctx). Three cycles of ctx with cisplatin and pemetrexed were administered, tumor objective response rate was assessed via CT-scan and the MPM was categorized as stable disease. After two consecutive applications, tumor progression was observed (Figure 2). After abstaining from debulking surgery, we initiated second line therapy with Ipilimumab and Nivolumab [5]. After six month of therapy, tumor masses showed an almost complete remission, but bullae like structures occurred between the pleura parietalis and visceralis (Figure 3). We assume that the rapid remission of the MPM lead to traction of the subpleural lung tissue as pleurodesis still had the lung attached to chest wall.
Conclusion
In conclusion, fast response of MPM treated with immunotherapy may result in emphysema like appearance due to the decreased elasticity of the lung and formation of bullae-like structures.
References
- Alchami FS, Attanoos RL, Gibbs A, Morgan F, Jasani B. Does Simian Virus 40 (SV40) Have a Role in UK Malignant Pleural Mesothelioma? No Role is Identified in a Sensitive RNA In Situ Hybridization Study on Potentially Affected Birth Cohorts. Applied immunohistochemistry & molecular morphology : AIMM. 2020; 28(6): 444-7.
- Robinson BM. Malignant pleural mesothelioma: an epidemiological perspective. Ann Cardiothorac Surg. 2012; 1(4): 491-6.
- Bibby AC, Tsim S, Kanellakis N, Ball H, Talbot DC, Blyth KG, et al. Malignant pleural mesothelioma: an update on investigation, diagnosis and treatment. Eur Respir Rev. 2016; 25(142): 472-86.
- Baas P, Scherpereel A, Nowak AK, Fujimoto N, Peters S, Tsao AS, et al. First-line nivolumab plus ipilimumab in unresectable malignant pleural mesothelioma (CheckMate 743): a multicentre, randomised, open-label, phase 3 trial. The Lancet. 2021; 397(10272): 375-86.
- Peters S, Scherpereel A, Cornelissen R, Oulkhouir Y, Greillier L, Kaplan MA, et al. First-line nivolumab plus ipilimumab versus chemotherapy in patients with unresectable malignant pleural mesothelioma: 3-year outcomes from CheckMate 743. Ann Oncol. 2022.