
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Delayed renal and liver laceration in patient with low velocity fall in setting of anticoagulation and renal mass: A case report
Brian M Thomas1*; Young G Son2; Benjamin A Fink1; Ian T Madison3; Ronald M Clearie2; Thomas J Mueller2
1 Department of Medical Education, Rowan University School of Osteopathic Medicine, USA.
2 Department of Urology, Jefferson Health New Jersey, USA.
3 Department of Clinical Education, Philadelphia College of Osteopathic Medicine, USA.
*Corresponding Author: Brian M Thomas
Rowan University School of Osteopathic Medicine,
Department of Medical Education, USA.
Email: thomas26@rowan.edu
Received : Apr 04, 2022
Accepted : May 02, 2022
Published : May 09, 2022
Archived : www.jcimcr.org
Copyright : © Thomas BM (2022).
Abstract
In this case report, we present a patient with a low velocity fall resulting in thoracoabdominal blunt trauma made occult by the absence of reported history or external physical signs and symptoms. Delayed grade 3 renal laceration and concomitant grade 2 hepatic laceration was the result in this patient that was being treated for septicemia in the setting of urinary tract infection, aspiration pneumonia, and anticoagulation for new-onset atrial fibrillation. This mismatch in initial presentation and severity of the delayed hemorrhagic process of multiple visceral organs after low-velocity blunt injury appears to be rare or significantly underreported. The acute decompensation and insidious course seen in this case highlights the importance of considering a more global assessment of hemorrhagic risk factors, rather than history, hematuria, and initial hemodynamic parameters alone.
Keywords: Renal laceration; Liver laceration; Hemorrhage; Fall; Anticoagulation; Renal mass; Trauma.
Abbreviations: EMS: Emergency Medical Services; g: Grams; dL: Deciliter; uL: Microliter; CT: Computed tomography; IR: Interventional radiology; cm: Centimeter; SCr: Serum Creatinine; IV: Intravenous; aPTT: Activated partial thromboplastin time; mmHg: Millimeters of mercury
Citation: Thomas BM, Son YG, FInk BA, Madison IT, Clearie RM, et al. Delayed Renal and Liver Laceration in Patient with Low Velocity Fall in Setting of Anticoagulation and Renal Mass: A Case Report. J Clin Images Med Case Rep. 2022; 3(5): 1824.
Introduction
Renal injury secondary to blunt trauma represents nearly 80% of all renal trauma and most often occurs secondary to high-energy events such as motor vehicle accidents, contact sports collisions, or falls from a height [1,2]. Notably, in trauma patients the mortality rate attributable to isolated renal injury is low as mortality is more often due to the large degree of associated injuries as one systematic review of traumatic kidney injuries reports a total mortality of 6.5%, with a renal injury specific mortality rate of 1.7% [3]. Even prior to the development of a formal organ injury scoring scale, it was understood that “significant” renal injuries, including lacerations and vascular injuries, account for 27-68% of patients with penetrating mechanism whereas blunt injuries only accounted for 4-25% of severe renal injuries [4-8]. Today, the organ injury scoring scale developed by the American Association for the Surgery of Trauma (AAST) scores significant injuries requiring surgical management for grades 4 and 5, and recommendations for surgical intervention for grade 3 renal injury exist only if undergoing laparotomy for other abdominal injuries already requiring surgical exploration [9-12]. A study of penetrating renal injury found that grades 3 through 5 were more associated with penetrating renal trauma, and furthermore, it is well established that higher grade, or more severe renal injury, is associated with necessity for more advanced interventions including nephrectomy [11,13-15].
Though mechanism and degree of trauma is associated with significant and higher grade renal injury, high-energy impact is not prerequisite for significant injuries and subsequent hemorrhage, especially in the structurally abnormal kidney [3]. indications to order imaging, computed tomography (CT) with IV (intravenous) contrast is recommended for its sensitivity, includes gross hematuria, hemodynamic instability (Systolic Blood Pressure < 90 mmHg) with microscopic hematuria, and/or history of traumatic mechanism or suspicious radiographic finding (rapid deceleration or spinal process fracture) [12].
Case presentation
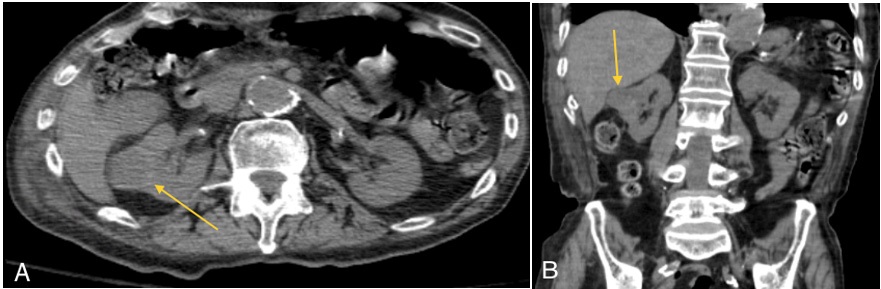
An 82-year-old male presented to the emergency department within one hour of onset of weakness and a fall from the toilet with assistance to the ground per family and Emergency Medical Services (EMS). Past medical history was significant for hypertension, chronic obstructive pulmonary disease, gout, and advanced dementia. He was found to have new-onset atrial fibrillation on electrocardiogram (ECG) with a maximum heart rate of 97 bpm, blood pressure 180/80, temperature of 97.8F (36.6C), and respiratory rate of 16. The patient’s white blood cell count (WBC) was 12.1 X 103 per uL (microliter), lactate of 6.6, serum creatinine (SCr) was 1.17, and his high-sensitivity troponin was 41. Due to his new-onset atrial fibrillation and his risk of stroke (CHADS2 score = 2), IV heparin drip per an aPTT-driven protocol for anticoagulation was started. A urinalysis (UA) demonstrated clear, yellow urine with 1+ protein, 3+ blood, >100 RBCs, >100 WBCs, many bacteria, negative nitrite, 2+ urine leukocyte, and subsequent urine cultures revealing >100,000 colony-forming units of Proteus Mirabilis. Blood cultures also found Gram-positive cocci. Ceftriaxone and clindamycin were started empirically. CT chest, abdomen, and pelvis without contrast revealed right lower lobe aspiration pneumonitis and a 3.3 cm right renal mass concerning for neoplasm and did not report hematoma or fracture other than a degenerative compression fracture of the L2 vertebra (Figure 1). The patient was admitted for observation of atrial fibrillation and the treatment of a urinary tract infection.
On the second hospital day, a supratherapeutic aPTT of >125 seconds was noted and adjustments were made based on nursing-driven hospital protocol.
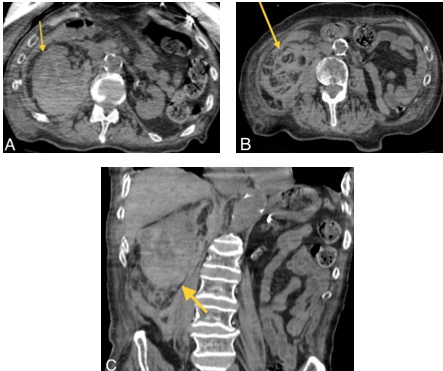
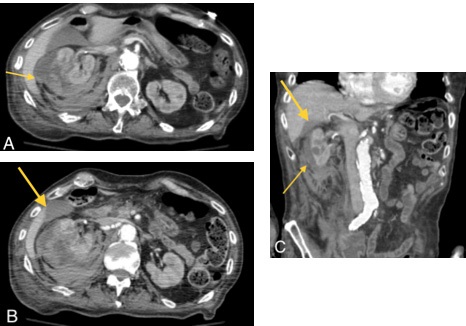
On the third hospital day, a decrease in hemoglobin from 8.2 to 5.9 g/dL (deciliter) (prompted the discontinuation of heparin protocol, administration of three units of packed red blood cells, and an upgrade to the intensive care unit. A CT chest, abdomen, and pelvis without contrast, due to the patient’s new severe acute kidney injury (SCr 3.2 from 1.17), found right renal hemorrhage with perinephric extension within Gerota’s fascia and in the posterior pararenal space (Figure 2). Healing fractures of the right 11th rib posteriorly with evidence of acute fractures involving the right 11th rib posteriorly and right 10th and possibly the 8th and 9th ribs laterally were also appreciated. Interventional radiology (IR) recommended repeat CT imaging with contrast to evaluate for active bleed and possible vessels for intervention. Repeat CT abdomen and pelvis with contrast displayed grade 3 right renal laceration with a stable right perinephric hematoma as well as a stable grade 2 liver laceration of the right hepatic lobe (Figure 3). An additional CT abdomen pelvis without contrast to determine collecting system injury revealed findings consistent with stable extensive right retroperitoneal hemorrhage with subcapsular, perinephric and pararenal components unchanged from previous CT as well as right renal and hepatic lacerations seen on previous contrast-enhanced CT. IR intervention for embolization and surgical intervention for exploration was discussed with the family. Further discussion with the patient’s family resulted in the decision for comfort care measures as the patient was a poor surgical candidate.
Discussion
There are few signs and symptoms well-associated with the presence or absence of renal injury. Those signs and symptoms are critically important for appropriate, guideline-directed selection of imaging studies and frequency [12]. Concomitant urinary tract infection in patients with suspected trauma can be misleading as it masks underlying potential renal injury. This case of a geriatric patient with urinary tract infection, pneumonia, and dementia, brings into question our reliance on the history and overt findings at the time of presentation. The case presentation is congruent with the mechanism of blunt renal injury, in which impact to the ribs or abdominal wall results in the kidney, anchored by the renovascular bundle and lying high and relatively protected in the retroperitoneum, collides with nearby structures such as the spine and deep back muscles [11,15]. This leaves hematuria with or without hypotension and a strong history of injurious process as the leading edge of the diagnostic plan. When the history is of poor quality and hematuria is suggested by other pathologic processes, as in our patient, it suggests that an assessment of the global risk factors for hemorrhage be considered.
The case presents several considerations for global risk factors of delayed renal hemorrhage in a patient with hematuria. The first risk factor is the presence of a pre-existing renal mass. Renal masses are the most common cause of non-traumatic spontaneous renal hemorrhage [16,17]. Furthermore, evidence suggests that pre-existing renal lesions increase the hemorrhagic vulnerability of the kidneys in blunt renal trauma [15]. The second risk factor predisposing this patient to progression of hemorrhage is anticoagulation. Anticoagulation increases the bleeding risk, even without any history of blunt trauma or fall; however, therapeutic anticoagulation would not be expected to be the sole cause of spontaneous renal hemorrhage. Of particular significance was the supratherapeutic nature of this course of anticoagulation that proximately preceded the hemodynamic instability that led this patient’s decompensation and clinical reevaluation. The third global risk factor to be considered is falls risk. The suspected impact in this patient, an assisted fall from toilet height--was sufficiently low energy that none of the historians characterized the event as traumatic. Though the susceptibility of the kidneys to injury increases in conjunction with impact velocity, as the injury threshold (specific energy density for rupture) decreases with increasing impact speed, a review of free-fall patients reported that severe renal injury did not correlate with the height of the fall and five of 24 patients with high-grade injuries had no hematuria [11]. This lack of correlation with impact and injury heightens the importance of any impact or fall history, no matter the perceived velocity, particularly when the patient is an adult older than 65 years old—a population in which one in four will experience a fall each year, accounting for nearly 36 million yearly falls in the United States [18].
Finally, a patient that presents with hematuria with any fall or traumatic mechanism where the history is not provided directly by the patient, as either a high-energy trauma, altered mental status, or, as in our patient, pre-existing dementia, high suspicion of blunt renal injury until appropriate imaging supports its absence. In this patient, who presented with a relatively benign physical exam—no ecchymoses, hematoma, or abrasions—and poorly characterized pain in the setting of dementia, a thorough history is important to develop a clinical plan. The perception of impact velocity was reported second-hand by caregivers and EMS to the best of their ability. In this case, the assisted fall from toilet height was perceived as sufficiently low-energy that none of the historians characterized the event as traumatic, supporting our proposal that any report of a fall from any height with the co-presentation of hematuria, regardless of other etiologic explanations for the hematuria, be investigated as a case of blunt renal injury.
Conclusion
This case represents a rare occurrence of concomitant hepatic hematoma and renal laceration secondary to a low-energy assisted fall causing trauma that was not appreciable on initial physical exam or imaging. There currently exists no other case reports in the literature that exhibit this unique co-presentation of grade 3 renal laceration and grade 2 hepatic laceration in the setting of low-energy blunt trauma. This multi-focal hemorrhagic process may represent a preponderance of etiological causes including the presence of a renal mass, supratherapeutic anticoagulation, and blunt trauma, but the patient’s clinical course may represent the ways in which causes of hematuria, other than blunt renal trauma, such as urinary tract infection can lead to a diagnostic workup that does not include the renal and hepatic injuries that were present in this patient. When the history is of poor quality and hematuria is suggested by other pathologic processes, as in our patient, it suggests that an assessment of the global risk factors for hemorrhage be considered in those patients who present with hematuria and are at risk of falls.
Declarations
Acknowledgements: None.
Funding: No funding to declare for this article.
Data access: All data pertaining to the case is included in the manuscript under the case presentation section.
Conflicts of interest disclosure: The authors declare no conflicts of interest.
Author contibutions
1. Brian M. Thomas, thomas26@rowan.edu - analyzed the patient data, wrote the preliminary draft, and read and approved the final manuscript.
2. Young G. Son, youngso@pcom.edu - analyzed the patient data, wrote the preliminary draft, and read and approved the final manuscript.
3. Benjamin A. Fink, finkbe86@rowan.edu - analyzed the patient data, wrote the preliminary draft, and read and approved the final manuscript.
4. Ian T. Madison, im7211@pcom.edu - provided expertise, edited the manuscript, and read and approved the final manuscript.
5. Ronald M. Clearie, clearier9@rowan.edu, ronald.clearie@ jefferson.edu - provided expertise, edited the manuscript, and read and approved the final manuscript.
6. Thomas J. Mueller, muellertj@gmail.com - provided expertise, edited the manuscript, and read and approved the final manuscript.
References
- Austin J, Rajkumar G. The diagnosis and management of renal trauma. J Clin Urol. 2018; 11(1): 70-76.
- Hotaling JM, Wang J, Sorensen MD, et al. A National Study of Trauma Level Designation and Renal Trauma Outcomes. J Urol. 2012; 187(2): 536-541.
- Petrone P, Perez-Calvo J, Brathwaite CEM, Islam S, Joseph DK. Traumatic kidney injuries: A systematic review and meta-analysis. Int J Surgery. 2020; 74: 13-21.
- Heyns CF, de Klerk DP, de Kock ML. Stab wounds associated with hematuria--a review of 67 cases. J Urol. 1983; 130(2): 228-231.
- Nicolaisen GS, McAninch JW, Marshall GA, Bluth RF Jr, Carroll PR. Renal trauma: re-evaluation of the indications for radiographic assessment. J Urol. 1985; 133(2): 183-187.
- Carlin BI, Resnick MI. Indications and techniques for urologic evaluation of the trauma patient with suspected urologic injury. Semin Urol. 1995; 13(1): 9-24.
- Bretan PN Jr, McAninch JW, Federle MP, Jeffrey RB Jr. Computerized tomographic staging of renal trauma: 85 consecutive cases. J Urol. 1986; 136(3): 561-565.
- Mee SL, McAninch JW, Robinson AL, Auerbach PS, Carroll PR. Radiographic assessment of renal trauma: a 10-year prospective study of patient selection. J Urol. 1989; 141(5): 1095-1098.
- Kozar RA, Crandall M, Shanmuganathan K, et al. Organ injury scaling 2018 update: Spleen, liver, and kidney. J of Trauma and Acute Care Surg. 2018; 85(6): 1119-1122.
- Gaillard F, Jones J. AAST kidney injury scale. Reference article, Radiopaedia.org. (Accessed on 05 Dec 2021) https://doi. org/10.53347/rID-1972.
- Santucci RA, Wessells H, Bartsch G, et al. Evaluation and management of renal injuries: consensus statement of the renal trauma subcommittee. BJU Int. 2004; 93(7): 937-954.
- Morey AF, Brandes S, Dugi DD. 3rd et al: Urotrauma: AUA guideline. J Urol. 2014; 192: 327.
- Santucci RA, McAninch JW, Safir M, Mario LA, Service S, Segal MR. Validation of the American Association for the Surgery of Trauma organ injury severity scale for the kidney. J Trauma. 2001; 50(2): 195-200.
- Wright JL, Nathens AB, Rivara FP, Wessells H. Renal and extrarenal predictors of nephrectomy from the national trauma data bank. J Urol. 2006; 175(3 Pt 1): 970-975.
- Kansas BT, Eddy MJ, Mydlo JH, Uzzo RG. Incidence and management of penetrating renal trauma in patients with multiorgan injury: extended experience at an inner city trauma center. J Urol. 2004; 172(4 Pt 1): 1355-1360.
- Zhang JQ, Fielding JR, Zou KH. Etiology of spontaneous perirenal hemorrhage: a meta-analysis. J Urol. 2002;167(4):1593-1596.
- Jha P, Saber M. Wunderlich syndrome. Reference article, Radiopaedia.org. (Accessed on 10 Dec 2021) https://doi. org/10.53347/rID-16265.
- Moreland B, Kakara R, Henry A. Trends in Nonfatal Falls and FallRelated Injuries Among Adults Aged ≥65 Years — United States, 2012–2018. MMWR Morb Mortal Wkly Rep. 2020; 69: 875-881.