
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Pathological profile of patients received for consultation in the dental unit of the Mbanga’s District Hospital
Esther Marguerite Chase Djanga*; Therese Mbezele Essomba; Vanina Doris Edo’O; Jules Julien Ndjoh; Jim Nemy Herve; Tatiana Mossus Etounou; Haamit Mahammat Abba-Kabir; Marie-Jose Essi
Professor, Department of Anesthesiology, Faculty of Medicine, Baskent University, Fevzi Cakmak Caddesi, Ankara, Turkey.
*Corresponding Author: DJANGA Esther MC
Yaounde Faculty of Medecine and Biomedical Sciences, Cameroon.
Email: e.djanga@yahoo.com
Received : Apr 05, 2022
Accepted : May 03, 2022
Published : May 10, 2022
Archived : www.jcimcr.org
Copyright : © DJANGA Esther MC (2022).
Abstract
Introduction: Oral health is a fundamental right for the individual regardless of age or living environment. Given the repercussions that the alteration of oral health could make in the daily life of an individual. It was a question in this work of determining the oral state of the patients of the dental unit in the District hospital of Mbanga.
Methodology: We carried out a cross-sectional descriptive study with an analytical aim carried out from April 12, 2021 to July 13, 2021 at the Mbanga District Hospital. It included any patient coming to consult the odontostomatology department who had given informed consent. A data sheet was used as a collection tool and data analysis was done on SPSS version 26.
Results: We had a sample of 81 patients with a sex ratio of 1.4. The average age was 35 years old with the extremes of 2 years and 81 years. The main reason for consultation was dental pain 40.7%. The caries risk was 4.07. We had 62.5% of patients over the age of 45 years old had poor oral hygiene. Up to 88.9% of patients required a scaling. It was revealed that 29.6% needed a dental prosthesis and 55.6% a dental extraction.
Conclusion: The oral state of the populations is approximate or even deleterious despite the presence of an equipped dental office in the locality. Action on certain determinants could positively influence the oral health of these populations.
Keywords: Oral health; Reason for consultation; CAOD; CPITN.
Citation: Djanga Esther MC, Essomba TM, Edo’O VD, Ndjoh JJ, Herve JN, et al. Pathological profile of patients received for consultation in the dental unit of the Mbanga’s District Hospital. J Clin Images Med Case Rep. 2022; 3(5): 1826.
Introduction
Oral health is an integral part of general health. It allows each individual to be able to interact with his surroundings. It is therefore fundamental for the development of everyone. In fact, the WHO defines oral health as the absence of oral or facial pain, oral or pharyngeal cancer, oral infection or lesion, periodontal disease, loosening and loss of teeth, and other diseases and troubles. This definition places oral health as a significant concept for the life of the person in the society [1]. On the other hand, it is observed in our societies that oral health is often neglected, yet oral diseases are very widespread, they concern all age groups, ranging from newborns to the elderly. They have both social and economic repercussions on the people affected [2]. Oral diseases affect more than 3 billion of people. About 2.3 billion of people have untreated dental caries on permanent teeth, more than 530 million children suffer from untreated dental caries on baby teeth, 796 million people suffer from periodontal disease. In some countries, considerable progress has been made in terms of prevention and quality of care. Despite this, the burden of oral diseases remains very high in some countries, especially developing ones, and often affects disadvantaged populations [3]. In Cameroon, there is very little data on the state of oral health, the most recent mentions dating from 1999 and there is no national oral health policy. However, it is obvious that there is an unequal distribution of human resources and an unavailability of material and financial resources in the Cameroonian health system, which makes it difficult to improve the management of oral diseases [4]. In the health pyramid, dental services are often more available at the central and intermediate level and less at the peripheral level [5]. This work therefore went to the Mbanga Health District, which is a District located in the Littoral region, to make an inventory of the oral health of the populations of this locality with a view to understanding how these populations manage their oral health. More precisely, it was a question of extracting the pathological profile of the inhabitants of this locality.
Materials and methods
Study type and site
We carried out a descriptive cross-sectional study for analytical purposes in the dental office of the Mbanga District Hospital. The study took place from April 14, 2021 to July 16, 2021 and data collection was made from May 22, 2021 to June 04, 2021. The study concerned all patients coming for consultation in the dental unit of the District Hospital of Mbanga. Included was any patient giving informed consent who could speak french or english. On the other hand, any patient who decided to withdraw from the study during its course or any patient whose examination could not be completed. After obtaining the various authorizations, we obtained the informed consent of the participants before subjecting them to the interview.
Tools and data collection
We used a technical sheet as collection tools divided into two parts. The first part concerned the identification of the participant, the second part concerned the examination and included the reason for consultation, the history, the exobuccal examination, the functional then intraoral examination next by the diagnosis and management. It was pretested in the same hospital. A health campaign was organized in view of the low attendance of the service for a period of one week. The participants came gradually and after giving their informed consent, the participant was seated on the dental chair in front of the investigator and the technical sheet was administered to him. The interviews took about ten minutes. At the end of the interview, counseling was given to each patient and for those wishing to receive care, a discount was granted on the care.
Data analysis
To perform the data analysis, we used the SPSS version 26 software. The input mask was made on Excel and the data were returned in the form of tables and graphs. The test used was that of Pearson’s Chi square and a difference was considered statistically significant for a value of p<0.05. For each participant, we counted the number of decayed, missing and filled teeth. From these values, the caries risk was found using the CAO index. The CPITN index was used to assess the periodontal profile of the participants as well as the Muhlemann classifications for mobilities and the Sillness and Loe classification for the plaque index.
Results
At the end of our work we obtained a sample of 81 particpants in this research work who fulfilled the selection criteria. The average age was 35.8 years and the extremes were 5 years and 81 years. The sex ratio was 0.8. The majority of patients were from the grass fields (40.7%), while we had 33.3% from the coast and 18.8% from the northwest and southwest. Only 3.7% were from central and northern Cameroon. The majority of participants were students (44.4%), there were respectively 14.8% civil servants, 11.1% retired patients and traders. 7.8% who lived from farming in the fields and 3.7% unemployed. The majority of the patients received lived in the city (81.5%), only 3.7% came respectively from Douala and Njombé. While 11.1% came from neighboring villages such as Mouyouka, Souza, Kompigna.
Regarding patient history 25.9% of patients had a medical history. These antecedents included patients with arterial hypertension, type 2 diabetes and epigastralgia whose etiology could not be defined. Most of the participants, around 74.1% of the candidates, had no ongoing treatment. The rest of the patients whose were under treatment were mainly taking analgesics and anti-inflammatories (gebedol, diclofenac, paracetamol) some of them said they were taking medication because of their clinical condition which covered a chronic pathology so there were some participants who said they were on antiretrovirals or on captopril for several years. Some 7.4% patients said they had allergies when taking the drugs. The only allergen listed here was aspirin. Patients said that ingesting this drug caused them either hot flushes or skin rashes or general malaise. Among the participants, only 7.4% said they regularly drink alcohol and sometimes smoke. More than half of the participants 59.3% came for their first consultation in a dental unit. Indeed, some patients said they did not consider it useful to come or never felt the need.
The main reason for consultation was dental pain in about 40.7% and quadrants 3 and 2 were the most cited as the quadrant bearing the causal tooth. The manifestation of pain varied from patient to patient. Some said they had pain at the site of the causal tooth, others spoke of radiating pain. Then, we found 29.6% of patients who came for a routine control, 11.1% came for a gene, gingival bleeding was found in 7.4% as well as dental fractures. Only 3.7% of patients consulted for cheek swelling.
The functional, exobuccal and endobuccal examinations revealed in 7.4% of the patients respectively a slurred speech, cheek swelling and finally swelling. gingiva next to the affected teeth. The rest of the participants did not present any particularity during the examination. Almost all of the patients had dental plaque. We found 44.4% of patients with a score of 2. While we found 29.6% and 14.8% of participants who had a score of 3 and 1 respectively according to the Sillness plaque index and Loe. Furthermore, concerning dental mobility, 3.7% of patients presented almost generalized and clinically detectable dental mobility. All of the affected patients were in the over 55 age group. Or half of these patients were affected by tooth mobility. The average CAD index was 4.07. The table below summarizes the CAOD and CPITN indices of the participants.
Table 1: Presentation of the CAOD and CPITN indices.
|
|
0-9 years |
10-15 years |
16-25 years |
26-35 years |
36-45 years |
≥ 45years |
||
CAOD |
C |
0 |
7.4% |
25,9% |
|
18.5% |
29.6% |
||
A |
0 |
0 |
3.7% |
7.4% |
3.7% |
11.1% |
|||
O |
0 |
0 |
0 |
0 |
3.7% |
0 |
|||
CPITN |
0 |
3.7% |
3.7% |
3.7% |
0 |
0 |
0 |
||
1 |
0 |
3.7% |
7.4% |
0 |
0 |
7.4% |
|||
2 |
0 |
0 |
14,8% |
7.4% |
14.8% |
7.4% |
|||
3 |
0 |
0 |
3.7% |
3.7% |
3.7% |
18.5% |
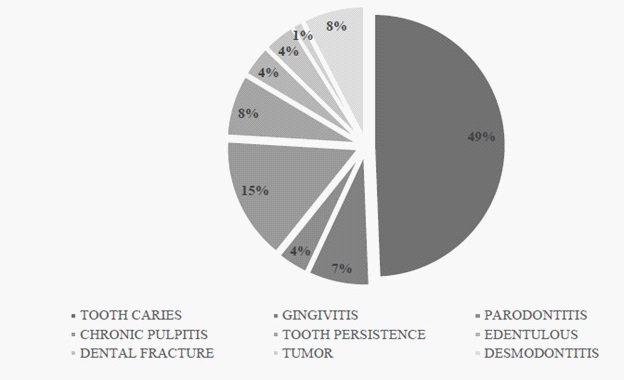
From this work, it appears that 11.9% of patients had no caries. But also only 18.5% of patients had a single cavity in the mouth. In 3.7% of participants, up to 9 decayed teeth were found in the mouth. Regarding missing teeth, 70.4% of participants had no missing teeth. While 18.5% had an absent dental organ. For dental fillings, only 3.7% of participants had working fillings. Regarding oral hygiene, 62.5% of patients aged over 45 had poor oral hygiene, 80% of those aged between 36 and 45 had average oral hygiene, while 75% of participants aged between 16 and 25 also had poor oral hygiene. average hygiene. Only participants under 9 years old had good oral hygiene. Oral hygiene deteriorated with age. The need for periodontal treatment was 88.9%. Indeed, these patients needed at least one scaling. Almost all patients over the age of 55 needed periodontal treatment. The diagnosis most frequently found among participants is dental caries and its various complications. We found in almost all patients 70.4% of patients a carious attack, followed by periodontal disease in 11.1% of patients. The following graph summarizes the diagnoses established in the patients of this study.
Apart from caries and periodontal conditions, other diagnoses were found such as dental fractures that were either coronary or more extensive reaching the vascular bundle of the pulp chamber. A case of benign tumor was also found, to be investigated to determine the nature of the tumor lesion. Some of the participants had come for the disfigurement of toothlessness. All of the children under 9 years old had lacteal persistence. Among those whose age group was between 10 and 15 years old, dental caries and its various complications were the main diagnoses. All age groups were affected by dental caries, periodontal disease affected participants aged 26 and over. Dental caries was found in almost half of the participants (48.1%). Among these patients affected by this pathology, more than half 53.8% came to a dental office for the very first time. It was also found that 22.2% of patients who came for a routine check had at least one cavity on one tooth, but also that 11.1% of participants with chronic pulpitis complained at the entrance to a odontalgia of quadrant 3. Tooth decay affected more than half 53.3% of the female participants.
Almost all of the patients needed care after diagnosis of the listed conditions. The prosthetic need at first glance concerned nearly 29.6% of the participants. Indeed, it was found that 22.2% needed to replace one or two missing teeth. Also, 75% of patients requiring a prosthesis had two teeth to replace. In the management of dental caries complications, 29.6% of participants required endodontic treatment. The most affected age group was between 16 and 25 years old where 37.5% of these patients needed root canal treatment. Regarding dental caries, 7.4% of patients had more than 9 decayed teeth in the mouth requiring conservative treatment. For scaling, it was found that the majority (81.5%) of the population needed at least one scaling session. More than half of the population 55.6% had exodontia in their care, 18.5% of participants had between 3 and 5 teeth to extract. Tooth extraction was the most common treatment given the vital prognosis of the tooth and the oral condition of the patients.
Discussion
The main limitation of this work is the low attendance of the odontostomatology department of the Mbanga District Hospital. Indeed, the average monthly attendance was around less than 15 patients per month. It is to compensate that we organized a campaign during recruitment.
We had a sample of 81 patients at the end of our collection, yet the locality of Mbanga is a cosmopolitan city with more than 25,000 inhabitants. The low attendance of health services in general and oral health in particular is a major challenge in public health. Populations living in rural areas are often less compliant with modern medicine. This could be explained by the fact that ethnomedicine would be more of a local medicine compared to modern medicine because it is more affordable financially and even socio-culturally. In a study on oral health behaviors and the determination of the use of oral care, conducted in 2013 in Dabou, Côte d’Ivoire, Sangare worked on individuals with various therapeutic choices. He found that in the first group where the therapeutic choice focused on contemporary medicine, the participants said they were more confident of modern medicine and that the dental offices were clean according to them, unlike the others who found that traditional medicine was the most suitable. because join the ancestral knowledge, it is less expensive, and the fact of the absence of pain during the treatment. We found a last group which chose to abstain from treatment, which it justified by the absence of financial means, self-medication or the perception of the non-necessity of care. The main determinant of this recourse was the educational level of the participants. This result is in line with our justification for the low attendance at the Mbanga dental practice [6].
The average age of the population was 35 years old, we found that 29.6% of patients were over 45 years old. Kane et al in 2018 in a similar study on the oral hygiene of patients consulting the odontostomatology department of a health center conducted in Mali found that the average age was 30 years [7]. In addition, Finance et al in 2012 had found that more than 50% of its study population was over 50 years old in its work on the attendance and satisfaction of patients in the odontology department of the University Hospital of Nancy [8]. We found that more than half of the patients received were female (55.6%). This result indicates that women are more concerned about their hygiene in general and oral hygiene in particular. Similar results have been found in several studies. In a study conducted in 2020 by Baba Diallo et al at the Bamako University Hospital, he found that of the 420 participants recruited, 52.1% were female [9].
Regarding the history of our patients, we had 25.9% who presented both medical and drug history. Among the drug history, the molecules mentioned by the patients (26.9%) were mainly analgesics and anti-inflammatories. Kaboré et al in 2016 in a study conducted in Ouagadougou on self-medication in odontostomatology found similar results, i.e. 30.4% of participants who mainly took paracetamol and sometimes antibiotics in their work [10]. This result on the use of self-medication as the first resort to care is in line with the study by Sangare et al in 2013, which found in a group of its participants that selfmedication was their therapeutic choice for several reasons, including the non-necessity of go to the hospital. For dental history, our study revealed that more than half of the participants (59.3%) received their first oral consultation [6]. Nokam et al had found a result a little less, i.e. 44% [11]. This difference could be explained by the fact that his study was carried out in an urban environment where the populations are more concerned about their oral health and have services nearby, while our study was carried out in a semi-urban or even rural environment where the conditions of life are not the same.
The main reason for consultation found in this study was pain for 62.9% of participants, it was mainly of dental origin in 40.7% of patients. Then, 29.6% came for a routine check-up and 7.4% for gum bleeding or a dental fracture. Berthé et al also found pain as the main reason for consultation in 78.2% of patients in their study on the reasons for consultation of patients in the Odontostomatology Department of Kayes Hospital in 2018 [12]. Then, the need of dental prosthesis for 5.4% of patients. Earlier, Ba M et al had conducted a fairly similar study in 2011 in Bamako, Mali and found that pain was the reason for consultation for 46.4% of patients followed by gingival bleeding in 31.4% of cases [13]. . Again, Tenebaum et al in 2015 had conducted a study on a younger population in the Pitié Salpêtrière hospital and found that 42.9% of emergency consultation cases were for pain related to a carious event [14]. Finally, Nokam et al in 2020 found in their research conducted on 325 patients in two public and private health facilities in the city of Yaoundé in Cameroon that the reason for consultation was pain in 78.2% of cases [11].
Oral hygiene in this research deteriorated with age. Indeed, while we found a fairly good oral hygiene in patients under 9 years old, it was found that 62.5% of patients over 45 years old had deleterious oral hygiene. In 2021, Fongoro et al in a study on a fairly similar population in Mali age groups found that 55.6% of participants had poor oral hygiene [15]. This result could be justified by the fact that his study population had a common defect which was the presence of diabetes. However, literacy has shown the clinical and statistical link between diabetes, which is a chronic disease, and the repercussions on the periodontium in particular. But still, Ba M had also found in his study population poor oral hygiene in 77.1% of cases while Kane in his research in 2018 in Mali found that almost all of his patients (91%) had a poor oral hygiene.
The CAOD was 4.07, which according to the WHO reflects an average caries index. Mindja et al in their study found a CAOD of 1.93 which is much lower than that of our study [16]. Finally, Moussa and Al had noted in their work on the oral health of patients hospitalized in a health facility that the caries risk was 2.52 results which is as close as possible to our research work [17].
Regarding the plaque index, it was average in 59.2% of the population and was worse in 29.6% of the population. Fongoro et al had meanwhile found an average plaque index in 52.3% of cases while Mindja et al had determined the value of the plaque index of his study population at 1.44 [15,16] .
The main pathology encountered was dental caries with a prevalence of 70.4%, which means that almost all of the participants had at least one cavity in the mouth and reflects the approximate oral status of the participants. Then we had periodontal disease with a prevalence of 11.1%. Kane in 2018 in Mali had found a prevalence of dental caries at 94.14%, not far Diawara O et al had found a prevalence of dental caries of 95% and an 87.8% prevalence of periodontal disease which he found in his research carried out in Bamako while Moussa only found a prevalence of dental caries in 63% of cases with 15.1% of periodontal disease [18]. This near similarity in these results could reflect a certain similarity in exposure to risk factors for oral diseases in the African region.
It was noted in this work that the management of oral diseases was diverse ranging from conservative care to dental extraction through scaling for periodontal diseases. However, the prosthetic need was significant. We found that 29.6% of the population needed at least one tooth replaced. Then 55.6% of the population needed tooth extraction and 29.6% of the population needed endodontic treatment and finally 81.5% of the population needed scaling. Nokam et al found in their work that 66.6% of participants needed tooth extraction while Fongoro et al found 58.7% of participants needed scaling. This result is almost identical to that obtained by Ba M et al who found a need for scaling in 57.5% of cases. For Kane et al, the majority of participants (91%) needed oral hygiene education [7]. These results show the need for large-scale care and the burden of oral diseases in our society.
Conclusion
It was a question in this work of determining the oral state of patients coming for consultation at the dental office of the District Hospital of Mbanga. It shows that the oral condition was deleterious because more than half of the population 70.4% had dental caries, and almost all of the participants 81.5% needed scaling. From these main results it emerges that the management of ailments oral health remains a public health problem even more in rural areas where action should be taken upstream by acting on the determinants of recourse and therapeutic routes because it was clear that patients went to a health facility as a last resort.
References
- World Health Organization. Oral health: key dental facts [Internet]. WHO. Sept 2018 [cited 2019 June 6]. Available from: http://www.who.int/mediacentre/factsheets/fs/fr/.
- WHO. Regional strategy for oral health 2016-2025: combating oral diseases as part of the fight against non-communicable diseases. Report of the seventy-sixth session. Addis Ababa: WHO. Africa Regional Office. 2016; 13.
- International Dental Federation (IDF). The FDI Global Vision 2020: A Prospect for the Future of Oral Health. FDI. Switzerland. 2012; 13.
- Ministry of Public Health. Health sector strategy 2016-2027. Minsanté; SOPECAM; Yaounde. 2016. 208.
- MINSANTE. Introduction of universal health coverage in Cameroon. Synthesis of the work of the national technical group. 2015; 38.
- Sangare AD. Oral health behaviors and determinants of healthcare use in the department of Dabou - Côte d’Ivoire. Human medicine and pathology. Claude Bernard University - Lyon I. 2011.
- Kane A.S.T, Guirassy M, Toure K, Diallo B, Diawara O, Sita-Cresp BLA, et al. Evaluation of the oral hygiene of patients consulting the odontostomatology department of the reference health center of Ouelessebougou in Mali. African J. of dentistry and implantology. 2020; 17: 22-32
- Finance B. Attendance and satisfaction of patients in the odontology department of Nancy University Hospital during the months of April and May 2012. Doctorate in dental surgery. Nancy, France: University of Lorraine. 2013.
- Diallo B, Toure SK, Diawara O, Coulibaly A, Traore A, Kane ST, et Al. Determinants of Attendance at the University Hospital Center-National Odontostomatology Center of Bamako CHU-CNOS. Sch J Dent Sci. 2021; 8(5): 118-23.
- Kabore W, Ouedraogo C, Konate A, Traore G, Chevalier V, Boismaré S. Self-medication during oral diseases in Ouagadougou, Burkina Faso. Oral Chi Oral Med. 2016; 22: 277-84.
- Nokam Abena ME, Gamgne C, Mengong H, Diffo RS, Bengondo C. Reasons for dental extractions in stomatology in Cameroon. Health Science and Disease. 2020; 21(8): 80-3.
- Berthé, D., Niaré, L., Sangaré M., Bamba S., Traoré A.A., Kané Aboubacar S.T. Reasons for consulting patients in the Odontostomatology Department of Kayes Hospital in 2018, Mali. Mali public health. 2020; 10(1): 79-83.
- Ba M, Diawaro O, Ba B, Niang A, Koita H, Toure A et Al. Contribution to the study of periodontal diseases in general practice: about 153 cases. African J. of dentistry and implantology. 2018;11 44-50.
- Tenebaum A, Sarric M, Bas A, Toledo R, Descroix V, Azogui-Levy. Consultation for oral emergency in children: retrospective study in France Elsevier. 2019; 1-32.
- Fongoro H. Evaluation of the oral status of diabetic patients in the dental office of the Diola reference health center: 63 cases. [PhD thesis in medicine]. Bamako, Mali: University of Sciences, Techniques and Technologies of Bamako. 2021.
- Mindja Eko D, Ngaba Mambo ON, Meva’a Biouele RC, Badamo Gnomo S, Ngo Nyéki AR, Mossus Y. Epidemiological and Clinical Profile of Stomatological Diseases in Patients Infected with HIV at the Regional Hospital of Maroua. Health Sci. Say. 2021; 22 (5): 80-4.
- Moussa M, Koumara A, Kolie A, Camara A. The oral health of patients hospitalized at the National Hospital of Niamey. Health Sci. Dis. 2021; 22(12): 132-4.
- Diawara O, Sidibe T, Ba B, Niang A, Ba M, Niang A, Ba M, Kane A, et al. Prevalence of oral and periodontal diseases among students in Bamako. Health Sci. Say. 2018; 19(2): 1-4.