
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A case of constrictive pericarditis after COVID-19 vaccine
Federico Cacciapuoti1; Paolo Tirelli2; Carlo Liguori2; Fulvio Cacciapuoti3
1 Department of Internal Medicine “L. Vanvitelli” University – Naples, Italy
2 Department of Internal Medicine and Radiology Unit “Ospedale del Mare”-Naples, Italy
3 Department of Cardiology-ICU “V. Monaldi” Hospital – Naples, Italy.
*Corresponding Author: Federico Cacciapuoti
Department of Internal Medicine, “L. Vanvitelli”
University of Campania, Italy.
Email: fulvio.cacciapuoti@gmail.com
Received : Apr 06, 2022
Accepted : May 03, 2022
Published : May 10, 2022
Archived : www.jcimcr.org
Copyright : © Cacciapuoti F (2022).
Abstract
It is known that mRNA vaccines against COVID-19 infection are effective in reducing symptoms, mortality and hospitalization of the patients suffering from COVID-19. In fact, these can cause some complications, as fever, headache, dizziness and, rarely, can induce some cardiac involvement, such as the inflammatory reaction of myocardium and/or pericardium. We describe a case of young healthy male-subject who received a second dose of Spikevax vaccine. Two days from the vaccine inoculation, he developed an acute inflammation of the pericardial leaflets, responsible for constrictive pericarditis. The clinical suspect was confirmed by instrumental and laboratory data. But, after the anti-inflammatory drugs administration, he completely recovered.
Learning objective: This case report describes the occurrence of constrictive pericarditis following the vaccination against COVID-19. The most common instrumental and laboratory texts, useful for the diagnosis, are illustrate. The therapeutic treatment are reported. The pathogenetic mechanisms are hypothesized.
Keywords: Vaccine; COVID-19; Constrictive pericarditis.
Citation: Federico C, Paolo T, Carlo L, Fulvio C. A case of constrictive pericarditis after COVID-19 vaccine. J Clin Images Med Case Rep. 2022; 3(5): 1827.
Introduction
The m-RNA vaccines (Cominarty and Spikevax) against Corona Virus Disease-19 (COVID-19) infection seems to be effective in reducing the symptoms related to the infection. But, the vaccines can frequently induce some adverse reactions, such as pain in the site of inoculation, headache, myalgia and, rarely, fever and/or Bell’s paralysis [1]. Acute myocarditis/pericarditis can also happen [2,3]. In particular, an increase in pericarditis rate was reported in young adults after the second dose of COVID-19 mRNA vaccines [4,5]. These inflammatory reactions are unchanged too, but could be referred to the immunopathological mechanisms due to the spike-protein involved in the COVID-19 infection [6]. That causes an imbalance of the ReninAngiotensin-Aldosterone System (RAAS).
Case report
A 32-year old man was admitted to the Emergency Room because of progressively worsening chest pain and dyspnea on effort started two days after the inoculation of the second dose of Spikevax vaccine against COVID-19.
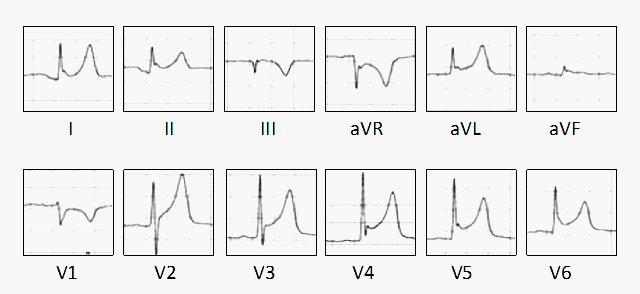
On physical examination, the jugular venous pressure was paradoxally increased on inspiration (Kussmaul’s sign). The peripheral blood pressure resulted of 130/90 mmHg, the heart rate was 91 bpm and the oxygen saturation of 98%. In addition, the body temperature was normal (36.5°C), while white blood test count increased (10.325/mmc) with 162.2% of neutrophils and 39.8% of lymphocytes. The inflammatory parameters and cardiac markers were both raised (HS-troponin=8 ng/L, fibrinogen=758 mg/dL). The first and second sound were present at cardiac auscultation, in absence of any systolic and/or diastolic murmurs. 12 leads-electrocardiography showed left axis deviation, and ST and PR depression, with normal T wave amplitude (Figure 1).
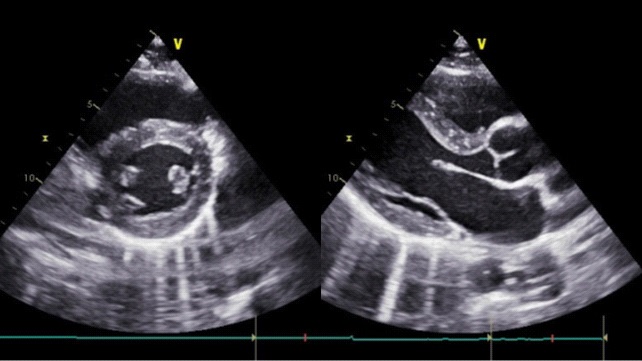
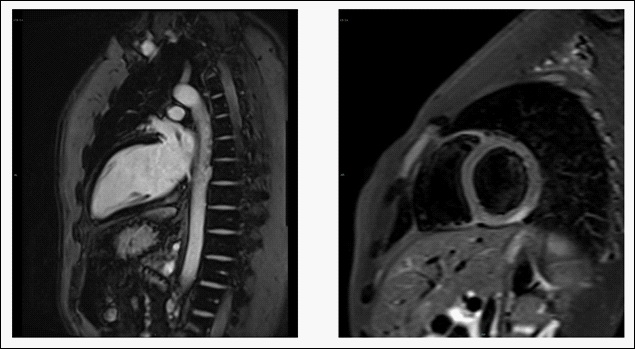
At chest radiogram no evident pleural effusion was reported, while the cardiac silhouette was in to the normal limits. Trans thoracic echocardiography (TTE) shown normal left ventricular diameters with normal systolic function and a moderate mitral regurgitation. A thickening of pericardial layers and numerous comets starting from thickened pericardium were seen [7] (Figure 2). The increased pericardial thickening, due to the inflammation of pericardial leaflets, is typical of constrictive pericarditis and is evident at cardiac resonance imaging (CMR) (Figure 3). The patient was treated with ibuprofen and colchicine [8] and completely recovered after 17 days, exhibiting a favorable clinical course, with cessation of all clinical symptoms and resolution of the other signs (ECG, TTE, CMR and laboratory texts).
Conclusion
The incidence of acute pericarditis related to COVID-19 vaccine inoculation is rather rare [9]. This post-vaccine complication is more frequent among adolescents of both sexes. Until now, no specific examination is available for its prediction. The diagnosis of constrictive pericarditis was performed for chest pain, cardiac palpitations, and dyspnea present at physical evaluation. It was confirmed by the characteristic findings at 12-leads electrocardiography found during the early phase of pericarditis. Usually, ECG changes of pericarditis evolve through four stages. At stage 1, ST tract and PR tract depression, with reciprocal changes are present (first week). T wave flattening is evident in the stage 2 (third week). The T flattening or its normalization continues in the stage 3 (after third week). In the final phase (stage 4) ECG returns to normal aspect [10]. Transthoracic echocardiography (TTE), with thickened pericardium and the characteristc comets, further documented the constrictive pericarditis. Finally, CMR definitely confirmed the diagnosis [11]. The immunologic reactivity to the vaccine’s content was hypothesized as a mechanism able to induce inflammatory reaction of pericardium to vaccine [12]. Really, various potential mechanisms were proposed, such as the hypersensitivity to vaccine, inflammatory reaction, excessive activation of immune system [13]. But, at moment, no specific mechanism was verified.
Conflict of interests: The Authors declare that there is not conflict of interest
References
- Anand P, Stahel VP. The safety of COVID-19 m-RNA vaccines: a review. Patient Saf. Surg. 2020; 30(141); 15. https://doi.10.1186/ s13037-021-00291-9.
- Sinagra G, Porcari A, Merlo M, Barillà F, Basso C, Ciccone MM, et al. Myocarditis and pericarditis following m-RNA COVID-219 vaccination. Expert opinion of the Italian Society of Cardiol. 2021; 22: 894-899.
- Luk A, Clarke B, Dahdah N, Ducharme A, McCrindle B, et al. Myocarditis and pericarditis after COVID-19 m-RNA vaccination: pratical considerations for Care Providers. Can. J. Cardiol. 2021; 37: 1629-1634.
- Pepe S, Gregory AT, Denniss AR. Pericarditis and cardiomyopathy after COVID-19 vaccination. Heart Lung Circ. 2021; 30: 1425- 1429.
- Nakanishi Y, Honda S, Yamano M, Kawasaki T, Yoshioka K. Constrictive pericarditis after SARS-Cov-2 vaccination: a case report. Am. J. Infect. Dis. 2022; 116: 238-240.
- Bettini E, Locci M. SARS-CoV-2 mRNA vaccines: immunological mechanism beyond 2021; 147. DOI:10.3390/vaccines9020147.
- Brandt RR, Ok J. Constrictive pericarditis: role of echocardiography and magnetic resonance imaging. E-Journ. Pratice 2017; 15, N° 23.
- Imazio M, Brucato A, Lazaros G, Andreis A, Scarsi M, Klein A, et al. Anti-inflammatory therapies for pericardial diseases in COVID-19 pandemic: safety and potentially. J. Cardiovasc. Med. 2020; 21: 625-629.
- Shimabukuro T. COVID-19 vaccine safety updates fda.gov. 2021 https://www.fda.gov/media/150054/download
- Imazio M, Gaita F. Diagnosis and treatment of pericarditis. Heart 2015; 101, 1159-1168.
- McReew A, Mergo P, Parihk P, Pollak A, Shapiro BP. Modern advances in cardiovascular imaging: Cardiac computed tomography and cardiovascular MRI in pericardial disease. Future Cardiol. 2014; 10: 769-779.
- Ramsamy V, Mayosi B, Sturrok E, Ntaehke A. Established and novel pathophysiological mechanisms of pericardial injury and constrictive pericarditis. World J. Cardiol. 2018; 10: 87-96.
- Hudon B, Mantooh R, DeLaney M. Miocarditis and pericarditis after vaccination for COVID-19. J. Am Coll. Emerg. Physicians 2021: 2. Doi:10.1002/emp2.12498.