
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
Aetiology in a female bronchiectasis patient presenting with shortness of breath
Shahina Akter, MD 1 *; Md Shahadath Hossain Towfikee 2 ; Tanjina Akhtar Banu 1 ; Md. Murshed Hasan Sarkar 1 ; Barna Goswami 1 ; Ahashan Habib 1 ; Salim Khan 1 , Khan Md Sayeduzzaman 3
1 Bangladesh Council of Scientific and Industrial Research, Dhaka, Bangladesh.
2 Saabiq Agro, Dhaka, Bangladesh.
3 United Hospital, Dhaka, Bangladesh.
*Corresponding Author: Shahina Akter
Principal Scientific Officer, Genomics Research
Laboratory, Bangladesh Council of Scientific and
Industrial Research, Dhaka, Bangladesh.
Email: shupty2010@gmail.com
Received : Feb 10, 2022
Accepted : May 04, 2022
Published : May 11, 2022
Archived : www.jcimcr.org
Copyright : © Akter S (2022).
Citation: Akter S, Towfikee SH, Banu TA, Sarkar MH, Goswami B, et al. Aetiology in a female bronchiectasis patient presenting with shortness of breath. J Clin Images Med Case Rep. 2022; 3(5): 1828.
Case background
The patient is 42 years of age, female presenting to the COPD department with acute pneumonia and shortness of breath. She had a history of granulomatous tubular formation (tuberculosis) in the lungs 10 years back. Then she has admitted in a hospital. After CT scan of the chest with contrast, the impression was, suggestive of bilateral pulmonary inflammatory lesions and left sided pleural effusion with thickening. Due to pleural effusion, thoracentesis has been performed to remove the fluid.
She reports excess sputum production but could not be managed to expectorate the sputum, chills, cough, chest pain, palpitations, fatigue, and in extreme conditions fever. Sometimes she felt severe weakness and sleepy. Her main problem is she reports difficulty breathing (shortness of breath) especially while speaking. At present she has experienced bleeding about 10-15 ml.
There are no known ill contacts at home. Her family history includes significant brain stroke disease and her father had shortness of breathing and her grandmother had sputum problem including sinusitis. She denies all smoking, alcohol and illegal drug use. There are no known foods, drugs, or environmental allergies.
Past medical history is significant for dyspepsia, sinusitis, COPD. Two times ruptured ectopic pregnancy and past surgical history of caesarean section (C-section) six years back. This study aimed to analyze the clinical records of the female with recurrent pneumonia in an attempt to identify factors that may lead to bronchiectasis (BE).
Bronchiectasis is a progressive respiratory disease characterised by permanent dilatation of the bronchi and associated with a clinical syndrome of cough, sputum production and recurrent respiratory infections [2]. Bronchiectasis is increasing in prevalence with current rates estimated between 53 and 566 cases per 100,000 inhabitants depending on the population studied [3,4].
Physical exam
Initial physical exam reveals temperature 98o F, heart rate 84 bpm, BP 110/70, HT 156 cm, WT 58 kg, BMI 23.8, chest tightness (occasional), throat pain (recurrent), chest pain (occasional) and O2 saturation 97% on room air.
Pulmonary/chest: Tachypnea present, respiratory distress (occasional), (+) wheezing noted, pleural effusion, PTB, chronic cough. The patient was barely able to finish a full sentence due to shortness of breath.
Cardiovascular: Normal rate, regular rhythm, and normal heart sound with no murmur. Lack of any edema sign.
Abdominal: Soft. Not too obese. Bowel sounds are normal. No distension and no tenderness are found.
Skin: Skin is dry
Neurologic: Awake, Alert, able to protect her airway. No sensation losses. Moving all extremities.
Evaluations
Initial evaluation to elucidate the source of dyspnea was performed and included CBC to establish if an infectious or anemic source was present, SGPT/ALT, sonography, S. Creatinine, RBS, S.IgE, C-reactive Protein (CRP), TSH, Anti-CCP, ANA/ANF, ECG, broncho-provocation test, chest X-ray, and CT-Scan.
CBC- Unremarkable and non-contributory findings to establish a diagnosis.
SGPT/ALT- within the normal range (18 U/L) S. Creatinine- within the normal range (0.9 mg/dl) Random Blood Sugar- 6.3 mmol/L S.IgE- within normal limit (21.0 IU)
Ultrasound report- liver, gall bladder, kidneys, pancreas, spleen, urinary bladder, uterus, adnexae etc. all are in normal size and position.
C-reactive Protein (CRP)- normal (<5.0 mg/L) TSH- 2.32 uIU/ml Anti-CCP- Non detected (<0.40 U/ml) ANA/ANF- negative (18.97)
Broncho-provocation test- Bronchoprovocation test is mildly Hyperresponsive Airways. An interpretation after this test are, C/C during the test: cough; Baseline Spirometry: Mild restriction; FEV1 is reduced by 17% at 25.0 mg/ml; reversibility: good
ECG
Normal sinus rhythm with non-specific ST changes in inferior leads.
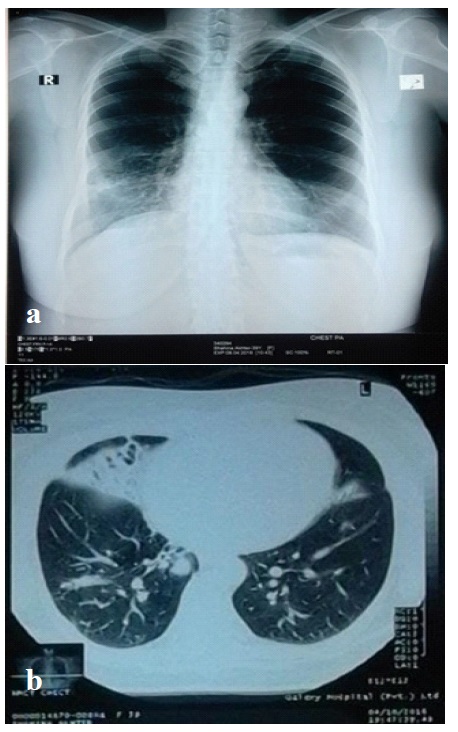
Chest X-ray Findings: Features are suggestive of the pulmonary inflammatory lesion (right). Pleural thickening/reaction (left)
Radiologist impression: Reticular/nodular opacities with suspected bronchiectasis inside. Chronic lung infection, inflammatory processes are possible. Minimal left basal pleural thickening. Right curvature of the thoracic spine. Deformity of lateral right 8th rib.
Confirmatory evaluation
The patient is getting sick again and again. Continuing to suppress the temporary disease through the application of antibiotics, but not fully recovering. His lungs become like honeycombs, giving way to all kinds of germs and thus getting affected. She got tested many times, but the reason for the disease remains unknown.
Testing was performed to include sputum AFB, sputum for gram stain, sputum for Eosinophils, GeneXpert detection of Mycobacterium tuberculosis, Mycobacterium tuberculosis complex and NTM, PCR (sputum), CT guided FNAC and CT scan of the chest. CT scan of the chest was investigated several times for anatomical abnormalities.
Sputum culture: Incubated aerobically at 37o C for 24/48/72 hrs; Z-N test- yielded no growth
Gram stain: Smear shows a moderate number of gram negative coccobacilli and pus cells/HPF.
Eosinophils: Eosinophils cells are not seen.
Xpert MTB/RIF: MTB and RIF both are not detected.
Mycobacterium tuberculosis complex: Negative Non-tuberculosis mycobacteria (NTM): Positive CT guided FNAC CT findings- A small soft tissue lesion is seen in the right middle lung along with the destruction of the rib. Aspiration Note- A needle is introduced. The needle tip is identified within the lesion. Aspirated a few drops of haemorrhagic material. No immediate complication is seen. Microscope description- Smear shows adequate cellular material containing plenty of degenerating polymorphs, lymphocytes and histiocytes in the background of extensive caseation necrosis. A few epithelioid cells are seen in the background. Dx- Lung middle right (CT guided FNAC): Granulomatous inflammation, tubercular
HRCT-scan of chest Multiple axial 2 mm HRCT Scan of chest were performed.
Findings
Increased attenuated areas having air bronchogram are noted in both medial and lateral basal segments of middle lobe and apical, posterior and lateral basal segments of right lower lobe. Few intervening cystic lucent areas are noted in medial basal segment of middle lobe. Multiple subpleural nodules and thickened septa and few nodules.
Impression: CT finding consistent with pulmonary inflammatory lesion with multifocal consolidation and bronchiectasis (right), possibly PT.
Treatment
Her medications include Azithromycin 500 mg, Levofloxacin 500 mg, Amoxycillin (500 mg) + Clavulanic Acid (125 mg), Doxycycline 100 mg, Moxifloxacin 400 mg, Clarithomycin 500 mg, Frabex 500 mg, Doxiva 200 mg, Provair 100 mg, Pantoprazol 20 mg, Salbutamol 100 mcg/puff, Salmeterol Xinafoate (25 mcg + 250 mcg/puff), Levocetirizine 5 mg. For PTB treated six months course. These drugs were given depending on the severity of the disease of patient [1].
Vaccinations
The patient was given Pneumovax 23 in every 5 years interval and Influvax every year.
Conclusion
The patient was suffering for a long time and had taken so many drugs as per the prescription of the physicians. In the sputum test, NTM had been diagnosed while Mycobacterium tuberculosis complex was negative. NTM are ubiquitous organisms in the environment and can be inhaled or ingested from water, soil and dust with different consequences according to individual and organism characteristics. According to the patient, she was not exposed to too much dust and she lead a very healthy life.
HRCT features were also investigated as NTM pulmonary disease was suspected. After HRCT scan of the patient confirmed the presence of bronchiectasis. Bronchiectasis is no longer a neglected disease. Discovering the underlying aetiology of bronchiectasis could make a real difference in the management and prognosis of patients and could delay the progression of lung involvement when treated. This female patient experienced the fact. She took lots of medicines given by her physicians who could not diagnose the disease accurately. During March April every year, her severity of disease increased. Currently, she feels better while taking Azithromycin 500 mg one day intervals along with montelukast 10 mg. Therefore, physicians should be familiar with her key clinical history and CT features that can raise the suspicion of a specific cause of bronchiectasis and lead to improved treatment.
References
- Bui PV. Disseminated Histoplasmosis with MiliaryHistoplasmosis, Neurohistoplasmosis, and Histoplasmacapsulatum Bacteremia in Probable Neurosarcoidosis. Case Rep Med. 2018: 3162403.
- Pasteur MC, Bilton D, Hill AT. British Thoracic Society guideline for non-CF bronchiectasis. Thorax 2010; 65: Suppl 1, i1–58
- Ringshausen FC, de Roux A, Pletz MW, et al. Bronchiectasis-associated hospitalizations in Germany, 2005–2011: a populationbased study of disease burden and trends. PLoS One 2013; 8: e71109.
- Quint JK, Millett ER, Joshi M, et al. Changes in the incidence, prevalence and mortality of bronchiectasis in the UK from 2004 to 2013: a population-based cohort study. EurRespir J 2016; 47: 186–193.