Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Atypical multifocal spinal tuberculosis mimicking malignancy on MR imaging
Anwesha D Patel
Meherbai Tata Memorial Hospital, Stocking Road, Bistupur, Jamshedpur, Jharkhand, 831001, India.
*Corresponding Author: Anwesha D Patel
Meherbai Tata Memorial Hospital, Stocking Road,
Bistupur, Jamshedpur, Jharkhand, 831001, India.
Email: dranwesha@gmail.com
Received : Apr 11, 2022
Accepted : May 06, 2022
Published : May 13, 2022
Archived : www.jcimcr.org
Copyright : © Patel AD (2022).
Abstract
Typical spinal tuberculosis affects the continuous vertebral levels and causes narrowing of the adjacent disc space and bone destruction. However, atypical form of spinal tuberculosis is difficult to distinguish from malignancy, leading to misdiagnosis and delay in treatment. Tuberculous spondylitis is a curable disease if permanent neurologic damage were avoided by early diagnosis and prompt treatment.
Citation: Anwesha DP. Atypical multifocal spinal tuberculosis mimicking malignancy on MR imaging. J Clin Images Med Case Rep. 2022; 3(5): 1832.
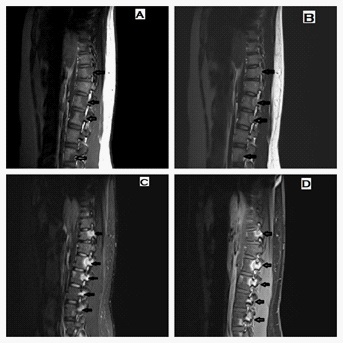
Clinical image description
Multilevel lesions of spine with sparing of intervertebral discs and absence of paravertebral soft tissue component is considered to favour neoplastic lesion whereas the presence of paravertebral lesion/collection favours tuberculous pathology. In our article, a19 year-old male presented with a 1-month history of low grade fever off and on; mild low back pain intermittently. Physical examination demonstrated no visible or palpable spinal deformity. Neurologic examination represented no specific findings. No other positive findings were found on physical examination. Laboratory investigations revealed red blood cells count, hemoglobin level, and white blood cells count were all within a normal range in spite of high erythrocyte sedimentation rate (ESR, 48 mm/hour), high C-reactive protein (66.9 mg/L). Computed tomography of whole spine images revealed no significant abnormality. Spinal magnetic resonance imaging (MRI) examination, showed mixed high-intensity changes at D11, L1, L2, L3, L4 ,L5, S1 and S2 levels involving the posterior aspect of body extending to the posterior elements; on T2 weighted (Figure 1B) and STIR images (Figure 1C) and decreased signal intensity on T1 weighted images (Figure 1A) with enhancement on postcontrast images (Figure 1D). Disc spaces, spinal canal and height of vertebrae were normal with no paravertebral collection. Bone marrow biopsy indicated a chronic granulomatous inflammation with abundant caseous necrosis, consistent with tuberculosis. Patient was started on ATT and the backache responded in four weeks with a repeat MRI after eight weeks of treatment revealing mild decrease in size of vertebral lesions. Therefore, a high index of suspicion is required for spinal tuberculosis even in atypical presentations and radiographic appearance, in areas with high endemicity of this infection.