
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Epidemiological profile of PLWH aged 50 and over at the Ahala district medical center, Yaounde
Thérèse Mbezele Essomba1,2; Vanina Doris Edo’o1,2; Marie Josiane Ntsama Essomba3 ; Marie José Essi1,2
1 Department of Public Health, Faculty of Medicine, and Biomedical Sciences, University of Yaounde I, Yaounde, Cameroon.
2 Laboratory of Research in Anthropology and Social Medicine, University of Yaoundé I, Yaoundé, Cameroon.
3 Geriatrics Department, Yaoundé Central Hospital, Cameroon.
*Corresponding Author: Thérèse M Essomba
Department of Public Health, Faculty of Medicine,
and Biomedical Sciences, University of Yaounde I,
Yaounde, Cameroon.
Email: mbezeleessombatherese@yahoo.com
Received : Apr 04, 2022
Accepted : May 09, 2022
Published : May 16, 2022
Archived : www.jcimcr.org
Copyright : © Essomba TM (2022).
Abstract
People living with HIV aged 50 years and over (P50+) represent a growing population in HIV care units in Cameroon. The objective of this study was to determine the epidemiological profile of this population in order to better target their management in HIV care units in Cameroon. It was found that the prevalence of P50+ was 13.3% and the median age was 58 [52-61] years. The sector of professional activity was dominated by the informal sector (45%), followed by unemployment (30%). The level of education was predominantly represented by secondary (52.5%) and primary (30%) education. The status of the partner was known in 67.5% of cases and 25% of partners were HIV positive. The median duration of HIV disease since discovery was 4 [3- 6] years. The circumstances of discovery were mainly clinical suspicion (67.5%). The most common type of HIV was type 1 (90%). The median CD4 count was 181 [9-319] cells/mm3 and 85.2% of patients had an undetectable viral load after at least 6 months of ART. The median duration of treatment was 48 [27-60] months and the 1st line of ART was used. The prevalences of hypertension, diabetes and renal failure were 24.3%, 7.5% and 23.1%, respectively. Other cardiovascular risk factors identified were physical inactivity (22.5%), excessive alcohol consumption (7.5%), and active smoking (5%). Electrocardiographic examination revealed the prevalence of rhythm, depolarisation, and atrioventricular conduction disorders in 11.4%, 5.7%, and 25.7% of patients, respectively. The prevalences of atrial and ventricular hypertrophy, repolarisation disorders, and myocardial ischemia were 37.1%, 5.7%, 8.6%, and 22.9%, respectively. The P50+ represent a distinct population within the PLWH with varied sociodemographic and clinical characteristics.
Keywords: HIV; Elderly; Cardiovascular health; Cameroon.
Abbreviations: GFR: glomerular filtration rate; CVRF: cardiovascular risk factor; PLWH: People living with HIV P50+ : PLWH of 50 years and over ART: antiretroviral treatment.
Citation: Essomba TM, Edo’o VD, Essomba MJN, Essi MJ. Epidemiological profile of PLWH aged 50 and over at the Ahala district medical center, Yaounde. J Clin Images Med Case Rep. 2022; 3(5): 1835.
Introduction
The Human Immunodeficiency Virus (HIV) infection has been of particular interest to researchers since its discovery and occupies a place of choice in world public health policies, this is explained by the evolution of its epidemiology. Indeed, according to the report of the Joint United Nations Programme on HIV/ AIDS (UNAIDS), the number of newly tested persons in the world rose from 3.4 million in 1996 to 5.4 million in 1999 and of all the registered cases of people living with HIV (PLHIV) in the world in 1999, 24.5 million were found in sub-Saharan Africa [1]. In Cameroon in particular, HIV prevalence increased from 0.5% in 1987 to 11.8% in 2002 [2]. To fight this pandemic which continues to decimate many communities with 32 million deaths in the world today, many strategies have been developed and implemented in a synergistic way on a global scale, the most recent of which is the one implemented by UNAIDS with the objective “95-95-95” to be reached by 2030 [1,3]. The impact of these interventions is quite palpable with the 2019 UNAIDS report which highlighted in 2018 a clear improvement in the figures with 1.7 million newly diagnosed people worldwide and in Cameroon, a prevalence of 3.6% among subjects aged 15-49 [4,5]. This suggests that the measures undertaken to put an end to the global scourge of HIV are bearing satisfactory fruits, placing it in the group of chronic diseases [6]. Moreover, with the advent of antiretroviral treatment (ART), PLWH now have a longer life expectancy [7,8]. We are therefore witnessing a decrease in the prevalence and incidence of HIV among young subjects and an increase in the latter among subjects aged 50 years and over: prevalence among these subjects is estimated at 14.1% in Cameroon [9-11]. This is partly for the reason mentioned above, but also because of the sexuality that is often ignored among older people who often neglect preventive measures against HIV infection [12-14]. PLWH aged 50 years and over (P50+) are therefore faced with new challenges related not only to age but also to HIV infection, including cardiovascular diseases [15-18]. In Cameroon, care for PLWH is provided in specialized services whose names vary according to the health facility where they are located, including the approved treatment center (ATC) and the care unit (CU). From all the above, it is necessary to know the profile of the P50+ followed in these different services, to better organize their management in the continuum of their care. The objective of this study was to determine the epidemiological profile of the P50+ followed up at the HIV care unit of the Ahala district medical center.
Materials and methods
Location and duration of the study
This was a situational analysis type study conducted from March 2021 to January 2022 at the HIV care unit of the Ahala district medical center, a 5th category health facility located in the 3rd district of the city of Yaounde, Cameroon.
Selection criteria
The study included all PLWH aged 50 years and over who were regularly followed up at the care unit.
Sampling and procedure
The sampling was consecutive. Recruitment was based on the medical records of PLWH followed up at the care unit department. After obtaining ethical and administrative authorizations and informed consent from the participants, sociodemographic, clinical (history of HIV infection), and paraclinical data (blood glucose, lipid profile, creatinin level with calculation of GFR according to the Cockroft and Gault formula, electrocardiogram) were collected.
Data analysis
The data were entered into CsPro 7.1 software and analyzed via SPSS 23 software. Because the data did not follow a normal distribution, quantitative data were expressed as median and interquartile range, whereas qualitative data were expressed as frequency and percentage.
Ethical considerations
This study was approved by the Ethics Committee of the Faculty of Medicine and Biomedical Sciences of the University of Yaoundé I (FMBS) and was conducted in strict accordance with the fundamental principles of the Declaration of Helsinki.
Results
Socio-demographic profile of the population
At the Ahala HIV care unit, 572 PLHIV are followed and 13.3% were P50+. The proportion of P50+ newly tested in the year of the study was 20%. The sex ratio male/female was 0.5 and the median age was 58 [52-61] years. The status of the partner was known in 67.5% of the cases and 25% of the partners were HIVpositive (Table 1).
Table 1: General characteristics of the population.
Variables (N=40) |
Categories |
Frequence |
Percentage |
Age (years) |
50-54 |
18 |
45 |
55-59 |
8 |
20 |
|
60-64 |
9 |
22,5 |
|
65-69 |
4 |
10 |
|
≥ 70 |
1 |
2,5 |
|
Marital status |
Single |
14 |
35 |
Married |
15 |
37,5 |
|
Common-law |
3 |
7,5 |
|
Widow(er) |
7 |
17,5 |
|
Region of origin |
Adamaoua |
2 |
5 |
Center |
31 |
77,5 |
|
North-West |
1 |
2,5 |
|
West |
4 |
10 |
|
South |
1 |
2,5 |
|
Southwest |
1 |
2,5 |
|
Level of education |
Not in school |
3 |
7,5 |
Primary |
12 |
30 |
|
Secondary |
21 |
52,5 |
|
Higher education |
4 |
10 |
|
Sector of activity |
Not employed |
12 |
30 |
Public sector |
4 |
10 |
|
Private sector |
1 |
2,5 |
|
Informal sector |
18 |
45 |
|
Retired |
5 |
12,5 |
Clinical and anthropometric data
The cardiovascular risk factors (CVRF) identified were physical inactivity (22.5%), hypertension (15%), excessive alcohol consumption (7.5%), active smoking (5%), and diabetes (2.5%). Clinical examination revealed a median body mass index (BMI) of 25.5 [20.3-29.7] kg/m² (Table 2). The waist-to-hip circumference (W/H) ratio was elevated in 21 (91.3%) women (W/H ≥0.85) and 6 (42.9%) men (W/H≥0.90). Elevated blood pressure figures were found in 9 (24.3%) patients and 3(6%) were known hypertensive. Fasting hyperglycemia was detected in 3 (7.5%) known non-diabetic patients.
Table 2: Anthropometric characteristics.
Variables (N=38) |
Categories |
Frequence |
Percentage (%) |
BMI (kg/m²) |
<25 (Normal) |
16 |
42,1 |
25-29,9 (Overweight) |
13 |
34,2 |
|
30-34,9 (Moderate obesity) |
8 |
21,1 |
|
35-39,9 (Severe obesity) |
1 |
2,6 |
Table 3: Paraclinical characteristics.
Variables (N=39) |
Categories |
Frequence |
Percentage (%) |
GFR (ml/min/1,73m²) |
≥90 |
9 |
23,1 |
60-89 |
21 |
53,8 |
|
30-5 |
9 |
23,1 |
Paraclinical data
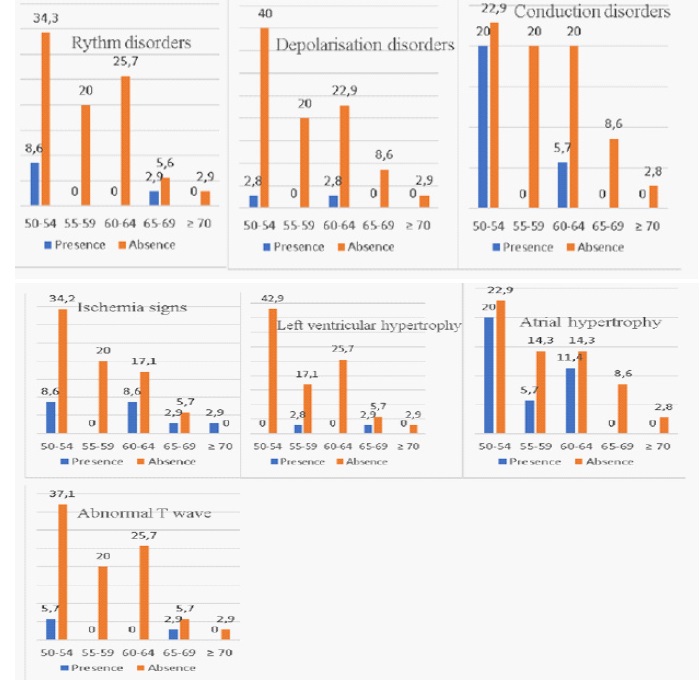
Kidney disease was detected in 9 (23.1%) patients with a GFR<60 ml/min/1.73m². Dyslipidemia with HDL (<0.4 g/l) was found in 5 (12.5%) patients and with LDL (>1.6 g/l) in 1 (2.5%) patient. Electrocardiographic examination revealed rhythm disorders in 4 (11.4%) patients and depolarisation disorders in 2 (5.7%) patients, atrioventricular conduction disorders such as bundle branch block in 9 (25.7%) patients, atrial and ventricular hypertrophy in 13 (37.1%) and 2 (5.7%) patients respectively. Repolarisation disorders such as abnormal T waves were found in 3 (8.6%) patients and signs of myocardial ischemia in 8 (22.9%) patients (Table 2).
Discussion
The proportion of P50+ and newly detected persons in this study was 13.3% and 20% respectively. This result is close to that of E.Eduard & al and R. A. Roomaney & al who respectively found a proportion of P50+ of 10% and 18.3% [19,20]. Furthermore, the Centers for Disease Control and Prevention (CDC) reports that in 2015, 47% of PLWH were aged 50 years and older and in 2016, 17% were newly screened [21]. These findings demonstrate that there is an increasing number of older PLWH in HIV services.
Secondary and primary education levels were the most represented in this research work compared to the R.A. Roomaney study (52.5% vs 42.1% and 30% vs 52.9%). This suggests that the majority of the P50+ population has a minimum level of understanding that could be an asset when implementing strategies to control certain diseases. The cardiovascular risk factors found were sedentary lifestyle (22.5%), kidney disease (23.1%), hypertension (15%), diabetes (7.5%), excessive alcohol consumption (7.5%), and active smoking (5%). These results are comparable to those of R. A. Roomaney & al who found prevalences of hypertension and diabetes of 38.2% and 7.8% respectively [20]. These results support the idea that P50+ have high prevalences of CVRF that make them vulnerable to cardiovascular diseases, which are responsible for 11-30% of deaths in PLWH [22].
The electrocardiographic abnormalities found are comparable to those reported by Y. Ding & al: rhythm disorders (11.4% vs 29.5%), conduction disorders such as bundle branch block (25.7% vs 0.9%), ventricular hypertrophy (5.7% vs 4.6%), abnormal T wave (8.6% vs 10.9%) and signs of ischemia (22.9% vs 0.4%) [23]. These results highlight the different types of cardiac dysfunction that are generally ignored by PLWH and that require specialized management and follow-up to reduce the mortality that could be related to them.
Conclusion
Ageing PLWH represent a significant and growing population in HIV care services. This could be explained by ART which efficiently reduces HIV-related deaths, increasing the life expectancy of this population. However, this population has several co-morbidities, including cardiovascular diseases. The question that arises is how these morbidities are managed in the continuum of care for PLWH.
Declarations
Funding: The researchers did not receive any external funding for this study.
Authors’ contributions: All authors contributed to the writing of this article.
Acknowledgements: We thank the participants in this study and all HI care unit staff of the Ahala district medical center.
References
- Programme commun coparrainé des Nations Unies sur le HIV et le SIDA. Rapport sur l’épidémie mondiale de VIH/SIDA juin 2000. Genève: ONUSIDA. 2000.
- Mossus-Etounou T, Essi M-JM, Isseini A, Souore-Sanda J, Pa’anaElemzo SB, Assala L-CB, et al. Evolution des programmes nationaux de lutte contre l’infection à VIH et le Sida au Cameroun, de 2000 à 2015. Health Sci Dis. 2016; 17(1).
- Bain LE, Nkoke C, Noubiap JJN. UNAIDS 90–90–90 targets to end the AIDS epidemic by 2020 are not realistic: comment on “Can the UNAIDS 90–90–90 target be achieved? A systematic analysis of national HIV treatment cascades”. BMJ Glob Health. 2017;2(2).
- Programme commun coparrainé des Nations Unies sur le HIV et le SIDA. Rapport sur l’épidémie mondiale de VIH/SIDA. Genève: ONUSIDA. 2019.
- Programme commun coparrainé des Nations Unies sur le HIV et le SIDA. Rapport sur l’épidémie mondiale de VIH/SIDA 2019. Genève: ONUSIDA. 2019.
- HIV/AIDS [Internet]. WHO | Regional Office for Africa. [cité 22 oct 2019]. Disponible sur: https://www.afro.who.int/healthtopics/hivaids.
- Life expectancy of individuals on combination antiretroviral therapy in high-income countries: a collaborative analysis of 14 cohort studies. Lancet. 2008; 372(9635): 293-9.
- Wandeler G, Johnson LF, Egger M. Trends in life expectancy of HIV-positive adults on ART across the globe: comparisons with general population. Curr Opin HIV AIDS. sept 2016; 11(5): 492- 500.
- Negin J, Gregson S, Eaton JW, Schur N, Takaruza A, Mason P, et al. Rising Levels of HIV Infection in Older Adults in Eastern Zimbabwe. PloS One. 2016; 11(11): e0162967.
- Wallrauch C, Bärnighausen T, Newell ML. HIV prevalence and incidence in people 50 years and older in rural South Africa. South Afr Med J Suid-Afr Tydskr Vir Geneeskd. déc 2010; 100(12): 812.
- Mbopi-Kéou F-X, Djomassi LD, Monebenimp F. Aspects descriptifs du VIH/SIDA chez les sujets âgés de 50 ans et plus suivis au Centre de Traitement Agréé de Bafoussam - Cameroun. Pan Afr Med J [Internet]. 2012;12.
- Rosenberg MS, Gómez-Olivé FX, Rohr JK, Houle BC, Kabudula CW, Wagner RG, et al. Sexual Behaviors and HIV Status: A Population-Based Study Among Older Adults in Rural South Africa. J Acquir Immune Defic Syndr 1999. 2017; 74(1): e9 17.
- HIV Prevalence and Sexual Behaviour at Older Ages in Rural Malawi. Jul 2012; 23(7): 490-496.
- Lebouché B, Wallach I, Lévy JJ. Vieillir avec le VIH : enjeux éthiques autour d’une population invisible. Éthique Publique Rev Int D’éthique Sociétale Gouv. 2008; 10(2).
- Alonso Alvaro, Barnes A. Elise, Guest Jodie L., Shah Amit, Shao Iris Yuefan, Marconi Vincent. HIV Infection and Incidence of Cardiovascular Diseases: An Analysis of a Large Healthcare Database. J Am Heart Assoc. 2019; 8(14): e012241.
- Barnes RP, Lacson JCA, Bahrami H. HIV Infection and Risk of Cardiovascular Diseases Beyond Coronary Artery Disease. Curr Atheroscler Rep. mai. 2017; 19(5): 20.
- Aberg JA. Cardiovascular Complications in HIV Management: Past, Present, and Future. J Acquir Immune Defic Syndr 1999. 1 janv. 2009; 50(1): 54 64.
- Boccara F, Cohen A. HIV and Heart Disease: What Cardiologists Should Know. Rev Esp Cardiol Engl Ed. 1 déc. 2016; 69(12): 1126 30.
- Eduardo E, Lamb MR, Kandula S, Howard A, Mugisha V, Kimanga D, et al. Characteristics and Outcomes among Older HIV-Positive Adults Enrolled in HIV Programs in Four Sub-Saharan African Countries. PLOS ONE. Public Library of Science. 2014; 9(7): e103864.
- Roomaney RA, van Wyk B, Pillay-van Wyk V. Aging with HIV: Increased Risk of HIV Comorbidities in Older Adults. Int J Environ Res Public Health. Multidisciplinary Digital Publishing Institute. 2022; 19(4): 2359.
- Aberg JA. Aging and HIV infection: focus on cardiovascular disease risk. Top Antivir Med. 2020; 27(4): 102 5.
- McGettrick P, Alvarez Barco E, Mallon PWG. Ageing with HIV. Healthcare [Internet]. 2018; 6(1).
- Ding Y, Zhu B, Lin H, Chen X, Shen W, Xu X, et al. HIV infection and electrocardiogram abnormalities: baseline assessment from the CHART cohort. Clin Microbiol Infect. 2020; 26(12): 1689.e1- 1689.e7.