
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Young stroke secondary to fibromuscular dysplasia causing carotid artery dissection
Rumesh Ranasinghe1; Shifa Azher1; Udaya Ralapanawa2; Parackrama Karunathilake2*
1 National Hospital Kandy, Kandy 20000, Sri Lanka.
2 Faculty of Medicine, University of Peradeniya, Peradeniya 20400, Sri Lanka.
*Corresponding Author: Karunathilake P
Faculty of Medicine, University of Peradeniya,
Peradeniya 20400, Sri Lanka.
Email: parackramawk@gmail.com
Received : Apr 09, 2022
Accepted : May 12, 2022
Published : May 19, 2022
Archived : www.jcimcr.org
Copyright : © Karunathilake P (2022).
Abstract
Background: Fibromuscular dysplasia (FMD) is a rare, medium-sized arteriopathy affecting less than 7% of the population. It affects predominantly young women of childbearing age. Stroke caused by fibromuscular dysplasia of the carotid artery is uncommon and reported to range between 0.6% by angiography and 1.1% by autopsy.
Case presentation: A 35-year-old mother of two children, previously well, was admitted to our hospital with right-sided spastic hemiparesis with upper motor neuron type facial nerve palsy. Non-contrast CT (NCCT) brain on admission revealed left-sided middle cerebral arterial territory infarction with possible hemorrhagic transformation with midline shift. She had progressive neurological features where NCCT brain in 24 hours showed an increase in the size of the hemorrhage. Magnetic resonance imaging (MRI) of the brain, including angiogram of neck vessels, revealed acute dissection of the left internal carotid artery with acute thrombosis, left frontoparietal hemorrhagic infarction, and the constellation of MRI showed features suggestive of left cervico-cranial fibromuscular dysplasia complicated by acute internal carotid artery dissection. She was started on low-dose aspirin, and 40 mg of atorvastatin and anticoagulants were not started because of the bleeding risk as she had a hemorrhagic transformation infarction. She was discharged and referred for inward physiotherapy and planned to repeat the MRI brain with the neck vessel angiogram in three weeks and arranged digital subtraction angiography in three months. Unfortunately, she was lost for follow-up.
Conclusion: Detailed evaluation of the young patients with ischaemic stroke is helpful to diagnose rare diseases such as FMD involving carotid arteries leading to a better treatment choice between anticoagulation vs. antiplatelet therapy
Keywords: Fibromuscular dysplasia; Stroke; Carotid artery dissection; Case report.
Abbreviations: MFMD: Fibromuscular dysplasia; NCCT: Non-contrast computed tomography; MRI: Magnetic resonance imaging; NIHSS: National Institutes of Health Stroke Scale; rTPA: Recombinant tissue plasminogen activator; WBC: White blood cells; Hb: Haemoglobin; MCV: Mean corpuscular volume; PLT: Platelets; ESR: Erythrocyte sedimentation rate; CRP: C-reactive protein; AST: Aspartate aminotransferase; ALT: Alanine aminotransferase; ALP: Alkaline phosphatase; INR: International normalized ratio; APTT: Activated partial thromboplastin time; UFR: Urine full report; RBC: Red blood cells; ACR: Albumin creatinine ratio; ANA: Antinuclear antibody; C-ANCA: Cytosolic antinuclear cytoplasmic antibody, P-ANCA: Perinuclear antinuclear cytoplasmic antibody; Antinuclear antibody; dsDNA: Double strand deoxyribonucleic acid; C3: Complement 3; C4: Complement 4; Anti-CCP: Anti cyclic citrullinated peptide; VDRL: Venereal disease research laboratory test
Citation: Ranasinghe R, Azher S, Ralapanawa U, Karunathilake P. Young stroke secondary to fibromuscular dysplasia causing carotid artery dissection. J Clin Images Med Case Rep. 2022; 3(5): 1841.
Introduction
Fibromuscular dysplasia (FMD) is a rare non-atherosclerotic, non-inflammatory angiopathy of medium-sized arteries [1]. It is commonly seen in females of childbearing age. The involvement of renal vasculature is 60%-75%, cerebrovascular 25%-30%, and visceral involvement is seen in 9% of people with FMD. Other than that, it could also occur in the coronary and pulmonary arteries and the aorta [2]. Clinical features of FMD depend on the arterial territory involved, but hypertension and stroke are the most typical clinical features encountered [3]. Cerebrocervical FMD can present as pulsatile tinnitus, headache, carotid bruit, and carotid artery dissection with stroke. For the diagnosis of FMD, contrast-enhanced CT and magnetic resonance angiography are the investigations of choice [4].
Case presentation
We report a case of a previously healthy 35-year-old mother of two children presenting with a stroke. She was relatively well before and developed sudden onset right-sided body weakness preceded by a headache while engaged in her routine household chores in the morning. She was taken to the local hospital and transferred to our unit on the same day. She had right-sided hemiparesis and slurring of speech on admission to the local hospital. National Institutes of Health Stroke Scale (NIHSS) was 6. Then after one hour from the onset of the symptoms, she developed global aphasia.
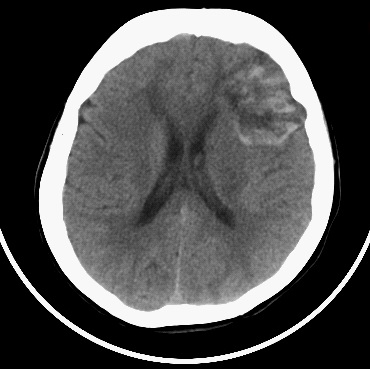
Non-contrast CT (NCCT) brain on admission to the emergency treatment unit revealed left-sided middle cerebral arterial territory infarction with possible hemorrhagic transformation with midline shift (Figure 1).
On admission to our ward, more than six hours had elapsed from the onset of the symptoms. She had right-sided spastic hemiparesis with upper motor neuron type facial nerve palsy, and other cranial nerves examination was essentially normal. Mild hypertension was the only vascular risk factor identified. There were no vascular bruits.
Because the risk of intracranial bleeding and the time for treatment with recombinant Tissue Plasminogen Activators (rTPA) had elapsed, it was decided not to give rTPA. As there were progressive neurological features compared to the admission, the NCCT brain was repeated in 24 hours, and it showed an increase in the size of hemorrhage compared to the previous CT scan. Magnetic resonance imaging (MRI) of the brain, including angiogram of neck vessels, revealed acute dissection of the left internal carotid artery with acute thrombosis, left frontoparietal hemorrhagic infarction, and concentric luminal narrowing of the left internal carotid, middle cerebral, and anterior cerebral arteries (Figure 2). Constellation of MRI showed features suggestive of left cervico-cranial fibromuscular dysplasia complicated by acute internal carotid artery dissection (Figure 3). However, a duplex scan of both renal arteries did not show any feature suggestive of renal artery stenosis. A summary of the other investigations done on this patient is shown in Table 1.
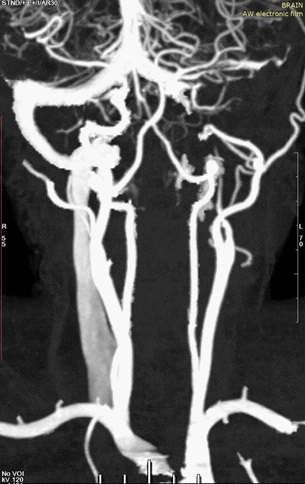
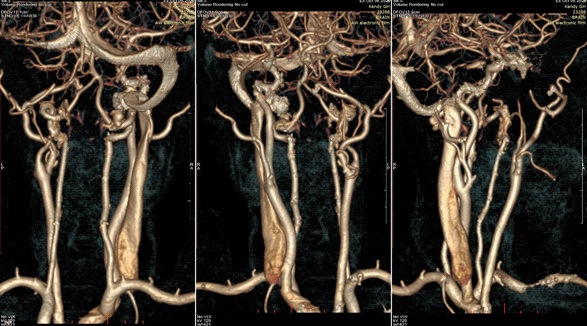
Table 1: Summary of the Investigations.
|
|
|
|
|
|
|
UFR
|
|
|
Her aphasia improved by 48 hours, and her weakness remained static throughout the ward stay. She was started on low-dose aspirin and 40 mg of atorvastatin. We opted not to start anticoagulants because of the bleeding risk as she had a hemorrhagic transformation of the large middle cerebral artery infarction.
She was discharged and referred for inward physiotherapy and planned to repeat the MRI brain with the neck vessel angiogram in three weeks and arranged digital subtraction angiography in three months. Unfortunately, she was lost for follow-up.
Discussion
Recent studies suggest that the incidence of fibromuscular dysplasia involving the craniocervical vasculature is less than 0.02% [2]. We are discussing a case of a 35-year-old female with fibromuscular dysplasia involving the craniocervical circulation who presented with an acute ischaemic stroke. The incidence of stroke in adults younger than 45 years ranges from 3.4 to 11.3 per 100,000 people per year [2].
Histology suggests that defective transformation of smooth muscle fibroblasts leads to degradation of elastic laminae, aberrant collagen synthesis, and segmental fibroplasia [4]. Unlike an atherosclerotic disease, fibromuscular dysplasia involves middle and distal arterial segments [5]. It could lead to arterial stenosis, occlusion, aneurysm, dissection, and arterial tortuosity. Smoking is now a potential contributing factor and portends a worse prognosis [2].
Although differential diagnoses for young females with stroke are vast, by the radiological imaging and the physical examination, the probable causes can be narrowed down where vasculopathy (such as arterial dissection), cardiac defects, recent pregnancy, other hypercoagulable states, smoking, illicit drug use, premature atherosclerosis, hypertension, low physical activity, metabolic disorders, migraine, and cases of focal cerebral arteriopathy need to be considered [6].
In this patient, non-contrast CT brain gave the first objective evidence of hemorrhagic infarction. The MRI angiogram of the craniocervical vasculature suggested vasculopathic etiology of fibromuscular dysplasia because of the apparent beading of the left internal carotid, middle cerebral, and anterior cerebral arteries. Fibromuscular dysplasia could be focal or multifocal. About 90% of patients have a multifocal disease, leading to the characteristic ‘string of beads’ appearance, which was seen in our patient. Although catheter-based angiography is considered the gold standard for diagnosis, it is not routinely practiced [3]. Digital subtraction angiography is performed with high clinical suspicion and to treat with revascularization for stenosis [6]. For FMD, there is no established corrective therapy up to date, but fortunately, it has a more benign course in asymptomatic individuals. Patients presenting with ischemic stroke should be evaluated to determine eligibility for reperfusion therapy with intravenous thrombolysis or mechanical thrombectomy [6]. Young stroke evaluation should include cerebral angiography to diagnose fibromuscular dysplasia and arterial dissection, vasculitis, and aneurysms, which are significant aetiologies for stroke in this population [3].
Management of cerebrocortical FMD mainly depends on the presenting symptoms and any associated neurologic complications such as carotid artery dissection, migraine, or aneurysm. Acute stroke in patients with FMD should follow standard stroke guidelines where it is not a contraindication to fibrinolytic therapy or mechanical thrombectomy in otherwise eligible cases. However, antiplatelet therapy may be preferred in carotid artery dissection because of safety and convenience, where studies have shown no benefit of anticoagulation over antiplatelet therapy [7]. Based on the clinical experience of the treating physician and other patient factors, comorbid conditions, and tolerance of these agents, the choice between antiplatelet and anticoagulation varies. Considering the risk of bleeding into the previous cerebral infarction with anticoagulation, we commenced antiplatelet therapy for our patient. Although a repeat imaging is suggested in three to six months to assess the status of the arteries affected by dissection, our patient defaulted the follow-up.
Conclusion
Detailed evaluation of the young patients with ischaemic stroke is helpful to diagnose rare diseases such as FMD involving carotid arteries leading to a better treatment choice between anticoagulation vs. antiplatelet therapy
Declarations
Ethics approval and consent to participate: Not applicable.
Consent for publication: Written informed consent was obtained from the patient to publish this case report and any accompanying images. A copy of the written consent is available for review by the journal’s Editor-in-Chief.
Availability of data and material: The data used during the current study are available from the corresponding author on reasonable request.
Competing interests: The authors declare that they have no competing interests.
Funding: This study was self-funded by the investigators. No external organization or institution was involved in this study.
Authors’ contributions: RR and SA analyzed and interpreted the patient data regarding FMD and subsequent management. All authors contributed to writing the manuscript. All authors read and approved the final manuscript.
Acknowledgments: We express our gratitude to the patient who kindly gave consent for this case to be presented in this paper.
References
- Putaala J, Metso AJ, Metso TM, Konkola N, Kraemer Y, Haapaniemi E, et al. Analysis of 1008 consecutive patients aged 15 to 49 with first-ever ischemic stroke: the Helsinki young stroke registry. Stroke. 2009; 40(4): 1195-203.
- Collins GJJ, Rich NM, Clagett GP, Spebar MJ, Salander JM. Fibromuscular dysplasia of the internal carotid arteries. Clinical experience and follow-up. Ann Surg. 1981; 194(1): 89-96.
- Ortiz-Fandiño J, Terré-Boliart R, Orient-López F, Guevara-Espinosa D, Ramón-Rona S, Bernabeu-Guitart M. [Ischemic stroke, secondary to fibromuscular dysplasia: a case report]. Rev Neurol. 2004; 38(1): 34–7.
- Olin JW, Sealove BA. Diagnosis, management, and future developments of fibromuscular dysplasia. J Vasc Surg [Internet]. 2011; 53(3): 826-836.e1. Available from: https://doi.org/10.1016/j. jvs.2010.10.066
- Puri V, Riggs G. Case Report of Fibromuscular Dysplasia Presenting as Stroke in a 16-Year-Old Boy. J Child Neurol [Internet]. 1999; 14(4): 233-8. Available from: https://doi. org/10.1177/088307389901400404
- Harriott AM, Zimmerman E, Singhal AB, Jaff MR, Lindsay ME, Rordorf GA. Cerebrovascular fibromuscular dysplasia: The MGH cohort and literature review. Neurol Clin Pract. 2017; 7(3): 225- 32.
- Fibromuscular Dysplasia and Stroke - Practical Neurology [Internet]. [cited 2021 Aug 21]. Available from: https://practicalneurology.com/articles/2020-jan/fibromuscular-dysplasia-andstroke.