
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
Urinary bladder tumour in a 10 years old child: A case report on urothelial papilloma
Naman Aggarwal1; Padmaraj Hegde1*; BM Zeeshan Hameed2; Prasiddh Hegde3; GVS Abhishek1; K Sricharan Raj1
1 Department of Urology & Renal transplant, Kasturba Medical College, Manipal Academy of Higher Education, Karnataka, India.
2 Department of Urology, Father Muller Medical College, Mangalore, India.
3 Department of Emergency Medicine, Kasturba Medical College, Manipal Academy of Higher Education, Karnataka, India
*Corresponding Author: Padmaraj Hegde
Department of Urology and Renal Transplant, Kasturba Medical College, Manipal Academy of Higher
Education, Karnataka, India
Email: padmaraj.hegde@manipal.edu
Received : Apr 18, 2022
Accepted : May 16, 2022
Published : May 23, 2022
Archived : www.jcimcr.org
Copyright : © Hegde P (2022).
Abstract
The suspicion and diagnosis of urothelial neoplasm are considered a rare commodity in the pediatric age group presenting with hematuria. A 10 years old patient presented to out-patient department with lower pain abdomen and hematuria for 2 months. Routine examination and ultrasonography, followed by urethrocystoscopy, revealed a solitary intravesical lesion in close approximation to the right ureteric orifice. Patient underwent transurethral resection of the bladder mass with histopathology confirming urothelial papilloma. This benign tumour is extremely rare in childhood with much to decipher of its etiology and further management.
Keywords: Hematuria; Pediatric age group; Urothelial neoplasm.
Citation: Aggarwal N, Hegde P, Hameed BMZ, Hegde P, Abhishek GVS. Urinary bladder tumour in a 10 years old child: A case report on Urothelial Papilloma. J Clin Images Med Case Rep. 2022; 3(5): 1848.
Introduction
There are not many emergencies more alarming than gross hematuria, for a urologist, presenting to the emergency triage. Most episodes of hematuria are signs of a urinary tract infection or a recently passed off urolithiasis [1]. But the presentation of gross hematuria warrants complete evaluation, regardless of age. Patients in their sixth or seventh decade of life are more likely to develop bladder urothelial carcinoma (UC). It has a lesser-known occurrence in children. Berrettini A found that they present in 1-2.4% of the population younger than 40 years, however, in the first two decades of life, UC is present as low as 0.1–0.4% population [2]. The literature on urothelial neoplasms in pediatric age group showed about 100 cases in the last century. The etiology, invasive potential, treatment, and surveillance strategy is not completely understood due to the rarity of pediatric UC [3]. We report a case of urothelial carcinoma of the bladder in a ten years old patient, highlighting the clinical presentation, diagnosis, treatment and follow up at our institute.
Case history
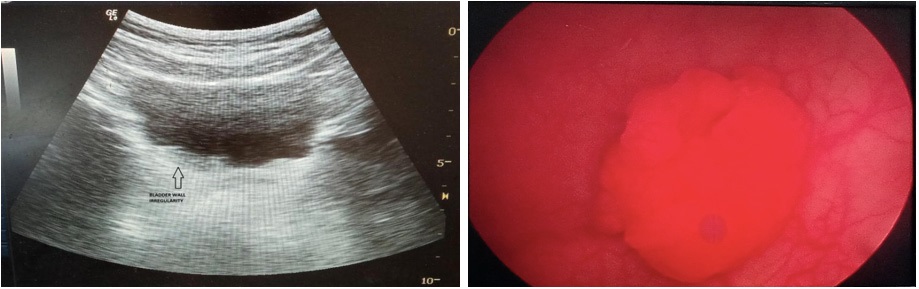
A 10 year old female patient was referred from community health centre in view of painful macroscopic hematuria to our institution for evaluation and further management. Her past history was nil significant for any type of benign urogenital diseases (UTI, urolithiasis etc), recent history of trauma or instrumentation. Family history was negative for any known tumors, including risk factors (smoking and alcohol). On physical examination, abdomen was soft and non-distended. No tenderness could be elicited on presentation. Ultrasonography was suspicious of bladder irregularity in the right lateral wall at the bladder trigone.
Due to irregularity and strong suspicion of bladder lesion, a diagnostic cystourethroscopy was conducted. Cystoscopy confirmed a small, about 1.5 cm papillary lesion growing from the right lateral wall, abutting right ureteric orifice. A formal transurethral resection of the bladder tumour was planned and conducted under general anaesthesia. Using 11.5 Fr cystoscope and monopolar cautery at 120/60 mJ energy setting, tissue specimen was retrieved and hemostasis achieved.
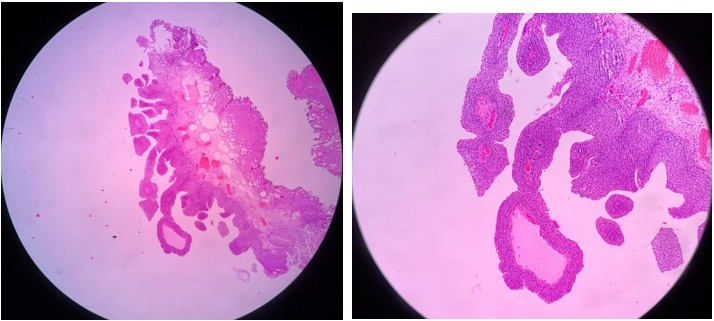
Histopathological examination showed a neoplasm with findings consistent of Urothelial Papilloma.
The post-operative course was uneventful. There was no recurrence of the hematuria. On follow-up at one month, laboratory, urine routine and microscopy tests and ultrasonography were done. All reports were within normal limit. Further plan is to evaluate patient at every 3-month interval.
Discussion
The epithelial tumours of the bladder rank amongst the top ten most prevalent cancer in the adult population. Contrary in the pediatric population, urothelial neoplasms are a rarely found. Fine et al surveyed surgical and histological information in regards to three pediatric urology unit’s cases, all younger than 20 years, and burdened with different types of urinary bladder neoplasms. Out of the 23 cases audited, 2 cases showed findings consistent with urothelial papilloma [3]. Between 1999 to 2013, “Berrettini et al studied the data in retrospect regarding urinary bladder tumours from three tertiary pediatric urology units. In consideration of the eighteen cases associated with bladder masses, only eight patients were diagnosed with urothelial papilloma” [2]. In terms of clinical presentation, the presence of gross hematuria has been reported in 80% of literature [4]. Urinary bladder tumours are typically associated with painless gross hematuria, our patient came with uncharacteristic painful macroscopic hematuria [2]. Urinary frequency, recurrent cystitis, pyelonephritis, obstruction, abdominal pain, flank pain, fever, hematospermia, nephrolithiasis, and emesis were among the numerous atypical presenting symptoms mentioned in the literature [5]. Detection of bladder mass on a routine ultrasound abdomen and pelvis has also been described [6].
In 2016, WHO classified tumours associated with the urinary bladder into carcinoma in situ, LGUC, HGUC, PUNLMP, UP, IUP, and urothelial hyperplasia and dysplasia [7]. In almost all of the cases, transurethral resection of the bladder tumour appear to suffice as a successful form of treatment [8].
At present, no defined guidelines have been formulated for follow-up for pediatric urothelial neoplasms. Urethrocystoscopy has proven to be the diagnostic investigation of choice for detecting recurrence of tumour [9]. Some authors suggest urine cytology and ultrasonography of the urinary bladder may be sufficient as screening test for low grade tumours such as papilloma [4]. “Bujons A postulated that urinary cytology has low- sensibility in detecting low-grade lesions in pediatric patients” [10]. The intensity of follow-up should be proportional to the risk of disease recurrence or progression [2].
Urothelial papillomas are a seldom found tumour entitiy, mostly in adult patient population. No consensus can be achieved on management of pediatric guidelines due to the small case load. An unknown risk of recurrence and progression of urothelial neoplasms in childhood demand a well-organized study to come to a conclusion for better management of pediatric subset of patients.
References
- Diven SC, Travis LB. A practical primary care approach to hematuria in children. Pediatric nephrology. 2000; 14(1): 65-72.
- Berrettini A, Castagnetti M, Salerno A, Nappo SG, Manzoni G, Rigamonti W, Caione P. Bladder urothelial neoplasms in pediatric age: experience at three tertiary centers. Journal of Pediatric Urology. 2015; 11(1): 26-e1.
- Fine SW, Humphrey PA, Dehner LP, Amin MB, Epstein JI. Urothelial neoplasms in patients 20 years or younger: a clinicopathological analysis using the world health organization 2004 bladder consensus classification. The Journal of urology. 2005; 174(5): 1976-80.
- Hoenig DM, McRae S, Chen SC, Diamond DA, Rabinowitz R, Caldamone AA. Transitional cell carcinoma of the bladder in the pediatric patient. The Journal of urology. 1996; 156(1): 203-5.
- Chu S, Singer J. Transitional cell carcinoma in the pediatric patient: a review of the literature. Urology. 2016; 91: 175-9.
- Marinoni F, Destro F, Selvaggio GG, Riccipetitoni G. Urothelial carcinoma in children: a case series. Bulletin du cancer. 2018; 105(6): 556-61.
- Humphrey PA, Moch H, Cubilla AL, Ulbright TM, Reuter VE. The 2016 WHO classification of tumours of the urinary system and male genital organs—part B: prostate and bladder tumours. European urology. 2016; 70(1): 106-19.
- Saltsman JA, Malek MM, Reuter VE, Hammond WJ, Danzer E, Herr HW, LaQuaglia MP. Urothelial neoplasms in pediatric and young adult patients: a large single-center series. Journal of pediatric surgery. 2018; 53(2): 306-9.
- Saltsman JA, Malek MM, Reuter VE, Hammond WJ, Danzer E, Herr HW, LaQuaglia MP. Urothelial neoplasms in pediatric and young adult patients: a large single-center series. Journal of pediatric surgery. 2018; 53(2): 306-9.
- Bujons A, Caffaratti J, Garat JM, Villavicencio H. Long-term follow-up of transitional cell carcinoma of the bladder in childhood. Journal of Pediatric Urology. 2014; 10(1): 167-70.