
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Intra osseous schwannoma of inferior alveolar nerve with multilocular radiolucency crossing the midline: A case report
Reju Sathar1*; Neelakamal Hallur2; Aaisha Siddiqua3; Chaitanya Kothari3
1 Senior Lecturer, AL-BADAR Rural Dental College & Hospital, Dariyapur, Naganhalli Road, kalaburagi, Karnataka, India.
2 Professor and Head, AL-BADAR Rural Dental College & Hospital, Dariyapur, Naganhalli Road, kalaburagi, Karnataka, India
3 Professor, AL-BADAR Rural Dental College & Hospital, Dariyapur, Naganhalli Road, kalaburagi, Karnataka, India.
*Corresponding Author: Reju Sathar
Senior Lecturer, AL-BADAR Rural Dental College &
Hospital, Dariyapur, Naganhalli Road, kalaburagi,
Karnataka, India.
Email: rju666@gmail.com
Received : Apr 18, 2022
Accepted : May 17, 2022
Published : May 24, 2022
Archived : www.jcimcr.org
Copyright : © Sathar R (2022).
Abstract
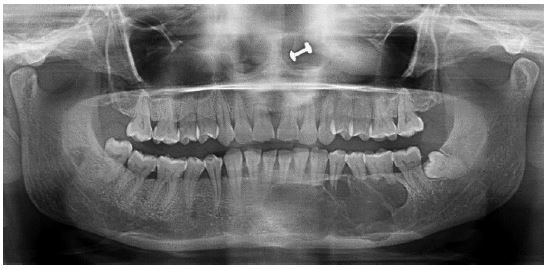
Schwanomma is a soft tissue tumor derived from Schwann cells of the peripheral nerves system. Schwannoma of the oral and maxillofacial regions primarily appears in soft tissue with tongue being the common site. Schwannoma arising within the bone are rare and commonly involve the mandible compared to maxilla. In this article, we report a case of rare intra-osseous schwanomma crossing the midline, which presented as a multilocular lesion on radiograph, which is again very rarely seen. Chief complaint of the patient was swelling and pain. Panoramic Radiograph showed a solitary oval shaped radiolucency with corticated borders and scalloping. Biopsy report revealed connective tissue component comprising of hyalinized stroma and tumor cells with large number of siderophages and histiocytes suggesting intra osseous schwannoma. Surgical resection performed and histopathologically examined confirming intra osseous schwannoma of ancient type. The post-operative course of the patient was uneventful for 2 years.
Keywords: Schwanomma; Ancient type; Inferior alveolar nerve.
Citation: Sathar R, Hallur N, Siddiqua A, Kothari C. Intra osseous schwannoma of inferior alveolar nerve with multilocular Radiolucency Crossing the Midline: A Case Report. J Clin Images Med Case Rep. 2022; 3(5): 1849.
Introduction
Schwannoma, also known as neurilemmoma or neurinoma, is typically, a benign soft tissue tumour derived from Schwann cells of the peripheral nerves system, which appears most frequently on auditory nerve [1-3]. Schwannoma of the oral and maxillofacial regions primarily appears in soft tissue [3]. Zhao Kun et al reported that tongue was the common site for occurrence in the 49 cases of neck and maxillofacial schwannoma [4]. Other common location in the oral cavity are Buccal mucosa, intramedullary bone of maxilla or mandible, floor of the mouth, palate, gingiva, lips and vestibular mucosa in that order [5]. Schwannoma arising within the bone are rare and account for <0.2% of all primary bone tumours [6] and this tumour arise most commonly in the mandible versus the maxilla [7]. The high frequency of mandibular involvement may be related to the presence of the inferior alveolar nerve, a sizeable, predominantly sensory nerve that traverses a long intra osseous canal [6]. No other bone contains a canal that transmits a neurovascular bundle of such size and length. The posterior mandible, where the canal is found, is the most frequent site of occurrence [8]. In this Article, We are reporting a case of rare intra osseous schwannoma crossing the midline, which presented as a multi-locular lesion on radiograph, which is again extremely rare.
Discussion
Schwannoma is an encapsulated benign neurogenic neoplasm that may develop in peripheral cranial or autonomic nerves and is composed entirely of schwann cells. Under normal circumstances, the latter are responsible for formation and maintenance of myelin sheath in the peripheral nerves. Sensory nerves preferentially develop schwannoma, presumably because they exhibit the highest (1:1) schwann cells to axon ratio [5,6]. The head and neck region is by far the most common site for schwannoma. The majority of it are encountered in the soft tissues and only rarely does the tumour arise within the substance of the bone [9]. Three mechanisms by which bony involvement can occur have been proposed;
1. A tumour can arise centrally within the bone. 2. A tumour can arise within the nutrient canal leading to the canal enlargement. 3. A soft tissue or periosteal tumour can cause secondary erosion and penetrate into the bone.
The first two mechanisms describe lesions that are truly intra osseous in nature however only schwannomas derived from the first mechanism are considered genuine primary tumors [10]. It is believed that, in the present case, one of the first two mechanism could be the cause of the bone involvement. There is an abundance of terms for schwannoma in the literature, which includes neurinoma, neurilemmoma and perineural fibroblastoma that has confused histological interpretation in the past and delayed accurate diagnosis [9,7]. The incidence of schwannoma is roughly equal in men and women, and most reports in the oral and maxillofacial region are in patients in their 20s and 30s, [11] and in the present case, patient was in her 40s, which is above the average age at which this rare tumor has usually been detected. Schwannomas are often difficult to diagnose as they do not have any characteristic identifying features [12]. The usual presenting symptoms of schwannoma is a slow growing mass. Pain and neurological deficient are uncommon but are suggestive of malignancy [13]. It occurs most commonly in the posterior region of the mandible moreover, this tumour is often ignored without subjective symptoms [14]. In our case, a slow growing swelling was the major concern of the patient with intermittent pain.
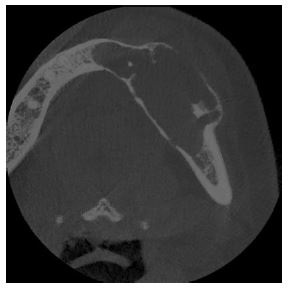
With regards to imaging data on schwannomas, radiographically, it is commonly unilocular and associated with resorption. It may resemble many types of benign or malignant conditions of the mandible such as odontogenic cyst, ameloblastoma and angioma, and if the tumor is large with cortical breaching it may resemble a malignant lesion. A potential radiographic clue to the diagnosis is the presence of a benign appearing lesion in the course of the inferior alveolar nerve [8]. Multilocular radiolucency with cortical expansion was observed in our case. CT Scan shows schwannomas to have an elliptical shape and clear boundaries, and have shown irregular peripheral enhancement (marked enhancement along the edges and non-uniform low density in the interior) and uniform enhancement (enhancement throughout the entire tumour) [11]. Similar findings were confirmed in the present case.
Microscopically, schwaannomas are typically characterized by frequent encapsulation, the absence of nuerities, and areas of Antoni A and B tissue occurring in variable proportions. Antoni A areas are relatively cellular and when more differentiated, may exhibit nuclear palisading, whirling and verocay bodies. In contrast Antoni B tissue is comprised of less cellular and less organised non organoid areas, often with prominent thickened blood vessels [7]. In addition to the classic schwannoma, several histopathologic subtypes exist. Usually large tumours of long duration having undergone degenerative changes such as cyst formation, haemorrhage and hyalinization are subtyped as ancient schwannoma [10]. Schwannoma with degenerative changes or ancient schwannoma are those displaying marked nuclear atypia of a degerative type. Large number of siderophages and histiocytes usually infiltrates the tumor itself. One of the most treacherous aspects of this tumor is the degree of nuclear atypia encountered. These tumors behave as ordinary schwannomas therefore nuclear atypia can be dismissed as a degenerative change [15]. Biopsy in the present case revealed degenerative changes with large number of siderophages and histiocytes confirming intraosseous schwannoma of ancient type.

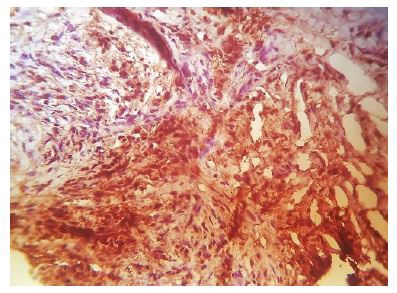


Schwannomas are not considered an aggressive neoplasm. Surgical excision with preservation of the neighbouring structrures and periodic follow up is considered the first line treatment of these lesions. Furthermore, radiatiotherapy is not adviced because the tumor is radio resistant [10]. The presence of verocay bodies and palisading nuclei with positivity on immunohistochemistry staining for S-100 protein confirms the diagnosis of schwannoma [14]. Our case shows similar findings on resected specimen with positive S-100 protein staining. There have been rare cases of recurrence of schwannoma in patients undergoing incomplete tumour extraction. Malignant transformation of the tumour is exceedingly rare [3]. Follow up of the present case for 2years has revealed no recurrence of the tumor.
Declarations
Conflicts of interest: None.
Funding: None.
Ethical approval: Not required.
Patient consent: Patient consent taken.
References
- Shetty SR, Rao PK, Chatra L, Shenai P. A case of a massive mandibular schwannoma. Journal of neurosciences in rural practice. 2011; 2(1): 65.
- Matsumine H, Sasaki R, Fujii K, Sakurai H. Intramasseteric Schwannoma Derived from the Masseteric Nerve. Plastic and Reconstructive Surgery Global Open. 2019; 7(3).
- Matsumine H, Sasaki R, Fujii K, Sakurai H. Intramasseteric Schwannoma Derived from the Masseteric Nerve. Plastic and Reconstructive Surgery Global Open. 2019; 7(3).
- Kun Z, Dao-Yi QI, Kui-Hua Z. A comparison between the clinical behavior of neurilemmomas in the neck and oral and maxillofacial region. Journal of oral and maxillofacial surgery. 1993; 51(7): 769-71.
- Arda H, Akdogan O, Arda N, Sarikaya Y. An unusual site for an intraoral schwannoma: a case report. American journal of otolaryngology. 2003; 24(5): 348-50.
- Ida CM, Scheithauer BW, Yapicier Ö, Carney JA, Wenger DE, Inwards CY, Bertoni F, Spinner RJ, Unni KK. Primary schwannoma of the bone: a clinicopathologic and radiologic study of 17 cases. The American journal of surgical pathology. 2011; 35(7): 989-97.
- Chi AC, Carey J, Muller S. Intraosseous schwannoma of the mandible: a case report and review of the literature. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 2003; 96(1): 54-65.
- Park YK, Kim YW, Yang MH, Kim EJ, Ryu DM. Neurilemmoma of the mandible. Skeletal radiology. 1999; 28(9): 536-9.
- Colreavy MP, Lacy PD, Hughes J, Bouchier-Hayes D, Brennan P, O’Dwyer AJ, Donnelly MJ, Gaffney R, Maguire A, O’Dwyer TP, Timon CV. Head and neck schwannomas–a 10 year review. The Journal of Laryngology & Otology. 2000; 114(2): 119-24.
- Perkins D, Stiharu TI, Swift JQ, Dao TV, Mainville GN. Intraosseous schwannoma of the jaws: an updated review of the literature and report of 2 new cases affecting the mandible. Journal of Oral and Maxillofacial Surgery. 2018; 76(6): 1226-47.
- Gotoh M, Ohnishi Y, Kubo H, Yamamoto H, Wato M, Morita S, Kakudo K. A case of schwannoma in the parotid-masseteric region. Journal of Oral and Maxillofacial Surgery, Medicine, and Pathology. 2014; 26(1): 92-5.
- Bansal V, Aggarwal P, Wadhwan V, Bansal A, Yadav M. Giant Solitary Schwannoma of Submandibular Salivary Gland—A Rare Entity. Journal of maxillofacial and oral surgery. 2017; 16(3): 382-6.
- Leu YS, Chang KC. Extracranial head and neck schwannomas: a review of 8 years experience. Acta oto-laryngologica. 2002; 122(4): 435-7.
- Kawasaki Y, Kobashi H, Ishii S, Yakushijib N. Intraosseous schwannoma localized in the anterior mandible with multilocular radiolucency: A case report. Oral Science International. 2016; 13(2): 37-40.
- Enzinger FM, Weiss SW, Goldblum JR. Soft tissue tumors. St. Louis: Mosby. 1988.